Editorial - Narratives of Essentialism and Exceptionalism: The Challenges and Possibilities of Using Human Rights to Improve Access to Safe Abortion
Alicia Ely Yamin and Paola Bergallo
Context
As this special section of Health and Human Rights goes to press, women’s access to sexual and reproductive health, including safe and legal abortion, faces both old and new threats in many corners of the world. Among other things, the US government under Donald Trump decided to defund the United Nations Population Fund and to reinstate and expand the so-called Global Gag Rule that prevents any non-US, nongovernmental organization from receiving funds from the United States if they provide not just abortion services but any information regarding abortion, even with other donors’ funds.1 USAID is the largest donor in the world for family planning services, and grantees will lose funding unless they agree to these conditions.2 As many as 50 European and other governments, including Canada, stepped in to try to make up at least in part for the loss in funding. Now that it has been announced that all US global health assistance funding for international health programs, such as for HIV/AIDS, maternal and child health, malaria, global health security, and family planning and reproductive health will be affected, the losses may be as much as US$9 billion.3
The funding crisis provoked by the new administration in the United States is but one facet of the challenges that the rapid ascendancy of conservative populist nationalism has created in relation to sexual and reproductive health and rights (SRHR), and abortion rights in particular. That is, the funding changes reflect the extreme degree to which ideology underpins policy in this area, domestically and globally, which advocates have long known. But after years of progressives using international forums to advance SRHR, including but not just abortion access, conservative actors have appropriated many of the same strategies based on an agenda that construes SRHR and “gender ideology” as fundamental threats to the traditional patriarchal family. These conservative actors seek not only to limit progressive advances in international law but also to undermine the legitimacy of the international institutions themselves and the norms that emanate from them. In the last couple of years, and especially the last year, the extent to which these conservative forces have consolidated transnational advocacy networks, and political blocs in international spaces, has become dramatically apparent, as evidenced by activity at United Nations (UN) forums as well as some of the transmissions of ideas across national contexts. Further, the de-legitimization of international institutions is mirrored at the national level with assaults on institutions of democratic governance, from the media to the courts, as shown by the actions of Trump (United States), Putin (Russia), Erdogan (Turkey), Orbán (Hungary), and others. SRHR are almost always among the first targets of these conservative populists, including abortion and extending to issues such as the traditional “family.”
At both the international and national levels, in parliaments and legislatures, there is increasingly little room for dialogue on issues relating to SRHR, including abortion. The impacts of this absence of dialogue are evidenced by, for example, limited, inconsistent, and regressive outcome documents and resolutions—from the Commission on the Status of Women to the Commission on Population and Development, from the UN General Assembly to the Human Rights Council. In this political landscape, we seem to have gone back to a time when human rights are universal only to the extent that they can be universally agreed on by member states. The construction of limited abortion rights under positive international law depended greatly on a normative scaffolding that now appears dangerously precarious.
The possibility of any meaningful collective deliberation regarding what is a contested issue in virtually every country of the world is further exacerbated by an all-out assault on scientific truth. The pseudo-science and alternative facts that are peddled cynically by opponents of choice—whether they relate to “fetal pain” or future suicide risks in women post-abortion—have proven remarkably influential over legislatures and courts in any number of countries. As the US Supreme Court found in 2016 in Whole Women’s Health v. Hellerstedt, the arguments used to support the “targeted regulation of abortion providers,” which called for requiring admitting privileges and “ambulatory surgical center” standards for abortion providers (requirements that, at the time, had been passed by more than a dozen US states), are also based on specious arguments.4
Not all is bleak in this picture, and increasingly the dynamics of different regions need to be considered separately to better understand how to move forward, as well as how to hold firmly onto what we have achieved. The Montevideo Consensus on Population and Development in Latin America, developed in 2013 as part of the International Conference on Population and Development (ICPD) plus 20 events, for example, stands out as a progressive beacon on issues of SRHR amidst a decidedly conservative global backdrop.5 Moreover, the African Commission on Human and Peoples’ Rights called for the decriminalization of abortion across Africa in both 2016 and 2017, in line with the Maputo Protocol to the African Charter on Human and People’s Rights.6
In any case, it is an especially apt time for scholars and practitioners across disciplines and geographic divides to collectively reflect on where we are in relation to using human rights discourse, tools, and framing to advance access to safe abortion as a right, and how we got here. The pieces in this special section of Health and Human Rights, which speak with multiple voices and perspectives on these complex struggles, are an important step in that direction.
Starting points
In the 1970s and 1980s, women’s rights activists around the world formed international and regional networks and developed feminist understandings of what began to be called “reproductive rights,” of which safe pregnancy and safe abortion were key elements. In the 1990s, women’s rights activists and scholars began appropriating international human rights forums and mechanisms to advance many issues in SRHR, including abortion rights, as well as other issues relating to gender equality, such as gender-based violence. The fall of the Berlin Wall and the subsequent erosion of rigid dichotomies between the West’s promotion of civil and political rights and the former Soviet bloc’s promotion of economic, social, and cultural rights seemed to signal an opening in international human rights law: the traditional dichotomies between the political and economic, and between the public and private realms in the traditional liberal state were challenged with new understandings of well-enshrined legal rights, and in turn rights-holders, as well as the nature of state obligations to them. International forums offered spaces to set standards and create consensuses that could not be achieved within the closed spaces of national legislatures and judicial systems.
A year after the World Conference on Human Rights in Vienna paved the way for women’s rights to be seen as human rights, the ICPD that was held in Cairo in 1994 was the culmination of years of activism and work on the part of women’s health and rights communities, together with LGBTQ and other communities. The Programme of Action that emerged from Cairo was a watershed, bringing into being a new paradigm of development based on women’s choices and reproductive rights. But we should not forget that “it was not all peace, love, rainbows and unicorns at Cairo.”7 Compromises were made, including around abortion. It was not just that pragmatism led to fissures among sexual and reproductive rights advocates but also that there were differing perspectives from women’s groups in the North and South, which would play out over the coming two decades.
At the time, many activists thought optimistically that ICPD meant that women’s movements had finally gotten a seat at the table, and that pushing further at the Fourth World Conference on Women in Beijing a year later in 1995—and across the intersectoral UN conferences of the 1990s—would allow more unified progress. In retrospect, the struggle had just begun, and the backlash against Cairo and Beijing, and SRHR, from right-wing governments, the Conference of Islamic States, the Vatican, and conservative evangelicals was still taking shape. Further, the identification of reproductive rights with autonomy in a vacuum in some countries, disconnected from the broader conditions in women’s lives, had consequences on the way alternative voices and movements for “reproductive justice” grew among women of color in the United States and elsewhere, for example.
The truth is that abortion was and is necessarily about reproductive, gender, and social justice and was recognized as such from early on in many countries, especially in the Global South.
It was and is about women and girls being fully human and therefore able to have control over their sexual and reproductive lives. And in many countries, SRHR activists recognized from the beginning of using rights paradigms for advocacy that decisional autonomy always required freedoms in the private sphere and access to social and economic endowments and entitlements in the public sphere.
At the end of the 1990s, despite the promise of “people-centered development” in the Millennium Declaration of 2000, the Millennium Development Goals (MDGs) returned to an essentialist view of women’s role in reproduction, including only one goal (MDG 5) on reproductive health relating to the reduction of maternal mortality (and in 2007 adding target 5B on access to “family planning”). Setbacks in certain regions after the fall of the Berlin Wall—such as in Eastern Europe, where there was a resurgence of Catholic conservatism—also created obstacles to women’s SRHR, and abortion in particular, in the 1990s. Indeed, it is often alleged that Poland was where the concept of “gender ideology” as a threat to the traditional family was initiated.
But legal mobilization for abortion and other SRHR moved ahead through the use of supranational tribunals and standard-setting, as well as at the national level. New generations of feminist lawyers availed themselves of advances in regional and international arenas, as well as structural innovations at the national level, such as constitutional blocs in domestic constitutional law in Latin America. Transnational advocacy networks created new geographies of knowledge, and the internet made the sharing of ideas and strategies among lawyers and activists in different regions infinitely easier. Lawyers worked with physicians and others to bridge gaps between normative victories and the effective enjoyment of rights in practice.
Today, it is clear that there is no one path forward, no one-size-fits-all strategy for achieving access to safe and legal abortion. Indeed, the articles in this issue, representing disciplines from the medical, social sciences, and legal fields, and a wide variety of geographical contexts, present a nuanced picture of struggles for abortion access using rights tools and frameworks. They also suggest, among other things, that we would do well to move beyond some of the standard debates in international human rights law in relation to abortion; promote more systematic intersectoral collaboration; focus on systems (both legal and health); and situate struggles within national and global political economies, and especially neoliberalism. The remainder of this editorial reviews the mobilizations and countermobilizations in different countries and across borders; sets out how a comprehensive and robust human rights-based approach (HRBA) would change conceptions of governmental responsibility and decisions within health systems; and, finally, notes the neoliberal economic context in which the regulation of women’s bodies and these debates are occurring.
Beyond the “legalism v. anti-legalism” debate in human rights scholarship
The topic of abortion ineluctably illustrates the hollowness of debates between legalism and anti-legalism in human rights scholarship, as well as epistemic dissonances between fields. Legalistic approaches to human rights and constitutional rights are often described as holding that ethical relations between people and, in the case of international law, states, are guided by rules which exist and are followed. With regard to abortion, many advocates would no doubt agree from an empirical perspective with Marge Berer that “the plethora of convoluted laws and restrictions surrounding abortion do not make any legal or public health sense. What makes abortion safe is simple and irrefutable—when it is available on the woman’s request and is universally affordable and accessible.” Yet in reality, exceptionalism and essentialism are the Scylla and Charybdis through which abortion reforms must be navigated. Law, of course, is not merely a set of rules but a reflection and refraction of negotiated social practices, and the validity of law is dependent on the process through which it is adopted. This is one of the things that makes abortion so contentious: it is notoriously impervious to forms of public deliberation, based on a shared understanding of empirical fact, which we expect from most of our lawmaking processes. This exceptionalism in lawmaking is coupled with widespread social norms that reflect and reinforce essentialism regarding women’s reproductive and caretaking roles in society.
A rigid legalism, which tends to see positive international law as well as domestic constitutions and legislation in formalistic terms, is justifiably critiqued as naïve by human rights scholars “[b]ecause rules do not, and cannot, constrain self-interested political actors.”8And, of course, laws do far more than set rules. Regarding abortion, it is especially clear that laws orient social norms and discourses, as well as reflect and reproduce gender relations.
In international law, the portrayal of a linear march of progress in a formalistic vision fails to consider the recursive relationship between international and domestic law, as well as considerations of normative and social legitimacy. As Johanna Fine, Katherine Mayall, and Lilian Sepúlveda’s paper shows, international and national human rights norms have interacted to create new interpretations of well-enshrined norms and to foster recognition of the denial of abortion care as a violation of women’s and girls’ fundamental human rights.
At the domestic level, too, there is no one-size-fits-all law reform or strategy for legal mobilization, as most of the papers show. A fundamental aspect of law that is well illustrated by this issue is that norms as written mean different things in different contexts, and a given law’s validity is contextual and the product of historical trajectories. In Chile, legal mobilization in favor of permitting abortion in case of fatal fetal anomalies (as well as on grounds of risk to life and health, and sexual assault) may today be the most strategic human rights move, as argued by Lidia Casas and Lieta Vivaldi, given the dynamics and history of Chile. In other countries, other strategies are required to ensure that rights are effectively enjoyed in practice at subnational levels, as Barbara Baird notes regarding Australia.
Across contexts, many of the authors implicitly or explicitly note the gap between normative symbolism and the “effective enjoyment of rights.” For example, Claire Pierson and Fiona Bloomer point to the limits of making effective change by framing abortion in terms of human rights recognized under international law in the context of Northern Ireland. They note that this strategy has not affected the macro-political level, where decision making takes place. Although in the Northern Irish context, rights have had high resonance in response to mainstream political conflict, they seem to be disregarded when it comes to liberalization of the abortion law.
Indeed, much legal mobilization now often incorporates an understanding of how de facto power relations structure the opportunities for women to avail themselves of abortion when it is legal. This important change in legal mobilization is illustrated by Ana Cristina González Vélez and Isabel Cristina Jaramillo in their documentation of the important work of Colombian women’s nongovernmental organizations seeking to shape the meaning of law through the development of legal expertise and pedagogical strategies to persuade health providers. Marta Rodriguez de Assis Machado and Débora Alves Maciel also recognize the significance of understanding power relations in the struggle for abortion reform in Brazil. In their paper, the authors trace the historical movement and countermovements deployed in different arenas, including the legislature, courts, and health authorities, since 1995, showing how legal progress is neither linear nor able to be understood without regard for the political context.
Lynn Morgan’s piece further underscores the importance of tracing conservative actors’ movements and the transnational networks they create, as well as the effects of conservative discourses. Morgan’s study of the Dublin Declaration on Maternal Healthcare and its deployment in abortion politics in El Salvador and Chile points to the array of conservative tactics faced by domestic advocates seeking legal reform or fighting arbitrary criminal law systems. Similarly, Julieta Lemaitre and Rachel Sieder explore how “legal mobilization before international human rights courts moderates social movement claims,” arguing that the international legal forum influences and alters the arguments of the actors before it, leading to moderated arguments by both feminist and conservative actors.
If Morgan’s and Lemaitre and Sieder’s pieces stress the transnational effects of advocacy, many of the articles describe how regulations have had differential impacts across countries, suggesting a need to develop strategies that go beyond national legislation and policies and work at the subnational level. This seems particularly clear in the articles about Australia, Thailand, and Nepal. As Ronli Sifris and Suzanne Belton’s work on Australia shows, in order for decriminalization to have a practical effect on women’s lives, the regulation of medical procedures and financial resources and the removal of legal and practical barriers are required at the subnational level to allow women to enjoy their rights. At the same time, in Thailand, where more moderate liberalizing interpretations of abortion law have been put forward, Grady Arnott, Grace Sheehy, Orawee Chinthakanan, and Angel Foster found variations in implementation conditions that have generated significant subnational disparities, with women from ethnic minorities in a border area receiving far more limited access to care.
Legal mobilization around abortion cannot be disconnected from the social contestation that occurs in other forums, beyond legislatures, courts, and administrative bodies, because this “societal legal mobilization” helps shape broader public understanding of the relationship between abortion and human rights. In her case study on Peru, Camila Gianella explores this “societal legal mobilization” in Peru’s two leading newspapers. Gianella observes legal mobilization and countermobilization through content analyses and thus captures the powerful narratives deployed in framing key concepts, such as conception, autonomy, vulnerability, and the social responsibility to protect.
Finally, there are cautions regarding the proliferation of norms and inconsistent use of legal tools in reproductive health. Jocelyn Viterna’s article on the process that led to defining abortion as aggravated homicide in El Salvador’s judicial system exemplifies the huge costs suffered most often by marginalized women and the abuse of the criminal law to regulate reproduction. Yet at the same time, we have seen a recent proliferation of obstetric-violence legislation in Latin America, which in the name of “protecting” women from abuses and mistreatment presents risks of drawing criminal law back into the reproductive health arena.9
Changing conceptions and decisions: Adopting human rights-based approaches more systematically in health systems
As noted above, the articles in this issue speak explicitly and implicitly to the need to go beyond law reform and litigation. The question is, how might HRBAs help us change the conceptualization of government actions and responsibility, as well as provide tools for advocacy around decision making at different stages of the health policy cycle, and beyond?
First, the way in which Zika was initially addressed in Latin America offers an example of how HRBAs might change thinking about state responsibilities. Zika is a disease of the poor, where standing water and inadequate housing create breeding grounds for mosquitoes. Zika was declared a public health emergency by the World Health Organization in 2016; and links between contracting Zika during pregnancy and serious congenital defects in the infant, including microcephaly, were established.10
At the time, various governments in Latin America, including Brazil, Colombia, Ecuador, El Salvador, and Jamaica, issued recommendations to women to postpone pregnancy for six months to “indefinitely.”11 From a human rights perspective, one problem with those official recommendations is that 56% of pregnancies in Latin America and the Caribbean are unplanned.12 Further, there is frequently inadequate or nonexistent comprehensive sexuality education; girls and women have little access to contraception; there is a very high incidence of sexual violence across the region; and there are cultural barriers to negotiating the use of condoms with male partners.13 Finally, many of the countries where these recommendations were made have partial or even total prohibitions on abortion.14 Thus, the way Zika was addressed, at least initially in some countries, exemplifies how marginalized women pay the greatest consequences for the political failures to enact public health measures or establish adequate health systems that meet the needs of poor women and girls.
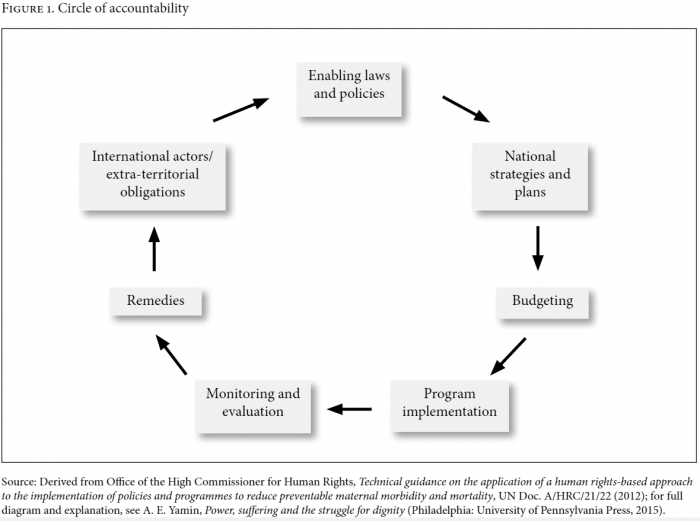
How does that change in thinking translate into action? Applying a systematic HRBA would change decisions (and advocacy opportunities around decision making) at every stage of the health policy cycle, as outlined in the UN’s 2012 technical guidance on a human rights-based approach to the reduction of preventable maternal mortality and morbidity (see Figure 1).15 This guidance was the first intergovernmentally approved document for a rights-based approach to any health issue—and one which is relevant to abortion at every stage.16
Joanna Erdman’s analysis of the different dimensions of time in abortion law argues that human rights law requires that limitations on abortion be “transparent, rational, and proportionate” and that a woman’s moral judgment to seek a later abortion be trusted. She argues that “international human rights law sets standards of legitimacy for abortion law as health regulation” and that laws should be “evidence-based to counter the stigma of late abortion.” She also convincingly argues that “there will always be a need for abortion services later in pregnancy” and that justice—and thus an HRBA—demands that structural limitations on women’s capacity to make earlier decisions on abortion be addressed. The paper by Casas and Vivaldi, about facing a diagnosis of fatal fetal anomaly in a setting where the law compels women to carry the pregnancy to term, offers an especially poignant example of the stark violation of women’s human rights and the difficulties faced by health professionals who can do little to ease women’s experience of loss and suffering in these circumstances.
Second, the effective enjoyment of all rights, including those related to safe abortion, requires multisectoral planning, and “linkages between sexual and reproductive health and related policies, including education and nutritional policy, should be drawn explicitly.”18 Arguably, planning should also include the regulatory approval of harm reduction strategies within and beyond health systems, even when many forms of abortion are illegal. And as Wan-Ju Wu, Sheela Maru, Kiran Regmi, and Indira Basnett note in relation to Nepal, to promote equitable access and safeguard abortion as a fundamental right, “policymakers must begin by including abortion as a part of the package of basic health care services and integrating safe abortion services into the continuum of reproductive health care.”
Third, budgets need to reflect these multisectoral plans and training for the providers involved across sectors. For example, Sifris and Belton explain that in Australia, the supply of public health facilities cannot meet the demand for services, thereby forcing women to seek services in the private sector. As a result, “there is a gradient of socio-economic access to reproductive health services that is inequitable.” This is common, even where abortion restrictions have been eased. Basnett also refers to the underfunding of abortions in Nepal. As the UN’s technical guidance explains, “The budget should ensure that financing is not borne disproportionately by the poor. Out-of-pocket costs cannot impede accessibility of care, irrespective of whether services are provided by public or private facilities.”19
Fourth, the implementation of programs, including regimes based on exceptions, requires the regulation of and protocols for provision and referral, and continuous training. For instance, the authorization of conscientious objection among health care providers when abortion is legal, and even more so when abortion is legally restricted, can be the source of important variations in women’s access to services. Wendy Chavkin, Laurel Swerdlow, and Jocelyn Fifield’s research outlines the necessary components for a functional health system that permits provider [conscientious objection] and yet assures access to abortion … : clarity about who can object and to which components of care; ready access into the system by mandating referral or establishing direct entry; and assurance of a functioning abortion service through direct provision or by contracting services to other abortion providers.
But the authors also make clear through an in-depth look at several countries that it is only in a few instances that this sufficiently protects women’s rights in practice.
Fifth, implementing an HRBA requires alignment between national policies and regulations and those of subnational states or provinces. Wu, Maru, Regmi, and Basnett argue that applying a human rights framework in Nepal would imply the need to “prioritize the decentralization of services and increase the number of health posts and sub-health posts with the capacity to provide first-trimester medical abortions,” invest “in technical support for providers in rural areas and referral networks to tertiary centers as needed,” and “safely expand the provision of second-trimester abortions.” Moreover, the importance of training pharmacy workers in Nepal and in other Asian countries with comparable conditions for the provision of medical abortion, such as Bangladesh, stretches the list of primary and community-based providers in the same way that contraceptive service provision has done.20
Sixth, the monitoring of abortion provision and post-abortion complications is extremely difficult where abortion is legally restricted. Nevertheless, monitoring that might enable evidence-based policies on abortion (or post-abortion care), assessment of legal compliance and institutional capacity, and status of conscientious objection, confidentiality, and the like—should be documented. Sifris and Belton discuss how the failure to collect and analyze health data “stymies the making of evidence-based clinical guidelines or health policies regarding elective abortion.”
Seventh, as discussed throughout the papers in this special section, remedies and litigation to transform legal regimes and to create new narratives of women as fully equal members of society are critical to protect this fundamental aspect of women’s dignity. Just as legalism alone is inadequate, simplistic anti-legalism does not reflect the advances made through a combination of national and supranational mobilizations, which have constructed normative understandings, exploited opportunity structures, and provided bulwarks against conservative political interests over time.
Finally, the context in which donors and development agendas shape what interventions are prioritized, as well as how services are organized and delivered, has enormous effects on abortion provision, especially in highly aid-dependent countries, as suggested by the discussion of funding at the opening of this editorial.
In short, a comprehensive HRBA in turn calls for a much greater interdisciplinary collaboration between the health and legal fields, as well as among scholars and activists in the social sciences. No one field alone can achieve normative victories and translate them into the “immanent regularity of practices,” as Pierre Bourdieu calls them, within health systems and larger cultures.21 And feminists should equally strive for men and providers to become allies in a broader social struggle for equal dignity in the communities and societies in which they live, which moves beyond both exceptionalism and essentialism.
Situating struggles for abortion and gender equality in a neoliberal world
It is very clear from the contributions to this special section that discourses at the global, regional, and national levels have an impact on the discourse and parameters for abortion advocacy. On one level, the Sustainable Development Goals (SDGs) are an enormous advance over the MDGs because they acknowledge the need for a universal framework—for rich and poor countries alike—and the need to look at inequalities within and between countries; and they also connect issues of SRHR with gender equality (and gender-based violence) and other pillars of development. For example, in the SDG framework, Target 3.7 (“universal access to sexual and reproductive health-care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programs”) is interdependent with “rights” under Target 5.6 (“universal access to sexual and reproductive health and reproductive rights as agreed in accordance with the Program of Action of the International Conference on Population and Development and the Beijing Platform for Action and the outcome documents of their review conferences”).22 Yet abortion did not make it to the indicators that will be used to measure achievements on these targets, and thus will likely fall through the proverbial cracks.
Further, it is clear from the diverse papers in this collection that achieving abortion access requires challenging not just ideological views of women as instruments of reproduction and caretakers of children but also views of women as anything less than full human beings with equal dignity and rights. It also requires subverting neoliberal fundamentalisms that increasingly control our collective imaginations.
The maintenance of the neoliberal status quo at the national and international levels is not compatible with a global system that recognizes and guarantees the effective enjoyment of substantive equality and social rights, including sexual and reproductive health rights. Market values influence all spheres of life in neoliberal economies, including how health systems are constructed and the very concept of health as a consumer good as opposed to a right or a tool for building a life of dignity. Liiri Oja’s research on Estonia discusses how although Estonia has a “good abortion law” that guarantees women timely and safe access to abortion, it is grounded in neoliberalism and therefore “important pillars supporting a steadfast reproductive rights protection remain missing,” particularly a “meaningful commitment to women’s reproductive rights and gender equality that protects women from shaming, micro-aggressions, and harmful stereotypes.” Baird’s paper on Australia exposes how the neoliberal environment characterizing the private supply of abortions in Australia explains the important subnational variations in access. Baird writes:
In the current neoliberal policy environment and in the context of continuing moral conservatism in Australia, [equitable access to abortion services] will only happen [when public health departments take responsibility and] under pressure of ongoing activism—and even then there are no guarantees.
Without effective regulation or public health care supply, the market delivers the illusion of freedom—the freedom of the consumer—while creating a reality of exclusion and degradation.
A number of the contributions in this special issue demonstrate the dangers of neoliberalism’s hegemonic grasp on development paradigms and social policies, which has had and will likely continue to have a disproportionately dramatic effect on women, who do not have the same access to education or paid work as men, and who depend on public health systems to a much greater extent. Further, the deep linkages between neoliberalism and the very plutocrats and nationalists that cynically decry it are related to other ideological and biomedical fundamentalisms that regulate women’s bodies. It is women who invariably experience the greatest marginalizing effects of neoliberalism, as well as the religious ideologies and biomedical hierarchies. The three tend to overlap when women are in contact with the health system due to socially constructed roles as caretakers, as well as their sexual and reproductive needs. Advocacy to emancipate women from one fundamentalism should draw links to others as well.
Concluding reflections
The most fundamental dilemma in promoting SRHR has been the tension between the need to protect women against violence (whether in the home or in war and crisis settings) and the need to empower them as autonomous agents with rights. The creation of binding norms and standards in SRHR is the product of years of work that recognizes that autonomy alone is not sufficient to guarantee substantive and material equality. Women require realization of the full spectrum of rights, including benefits to education, employment, and equal protection in addition to access to health care. Women require these freedoms and rights to be able to undertake their life projects and participate as full members of the communities and societies in which they live and to which they contribute.23
The infiltration of fundamentalist religious sects in representative politics around the world poses extraordinary risks to the realization of women’s rights when deliberative democracy functions in ways that impede impartial discussion of issues such as abortion and emergency contraception. But the pieces in this volume suggest that women face multiple fundamentalisms—which are connected. The fundamentalist religiosity is often allied with conservative nationalism that denies scientific truth. At the same time, neoliberalism commodifies women’s bodies, as well as access to care, in increasingly marketized societies. Indeed, the “de-defining” of the public and private realms—where women and girls voluntarily commodify themselves on social media spaces that are widely viewed but privately owned—and its impacts on women’s sexual and reproductive rights call for greater understanding.
Notwithstanding the progress that has been made, the issue of abortion may indicate most dramatically how deeply rooted and normalized patriarchy remains in our institutions and in our collective psychology. The autonomy to exercise control over our bodies—to have sexual relations when and with whom we want, without having to procreate—evokes discourses of uncontrolled selfishness and immoral hedonism about women.24 Until all women—poor and rich, disabled and able-bodied, young and old, of all classes, races, and ethnicities, and of all gender expressions and sexual orientations—are understood to have rights to sexual pleasure, which men take for granted, we will always be fighting defensively against restrictions that regulate our bodies, our desires, and in many cases our lives.
Acknowledgments
We are grateful to Marge Berer for her comments; her views are set out in the discussion piece that follows the editorial. We are also grateful to Angela Duger, research associate at Georgetown’s O’Neill Institute, for her assistance in the preparation of the editorial.
Alicia Ely Yamin is a visiting professor of law at Georgetown University Law Center and director of the Health and Human Rights Initiative at the O’Neill Institute for National and Global Health Law; adjunct lecturer on law and global health at the Harvard T.H. Chan School of Public Health; and a global fellow at the Centre on Law and Social Transformation. She currently serves as a commissioner on the Lancet-O’Neill Institute Commission on Global Health and the Law and the Independent Accountability Panel for the UN Secretary-General’s Global Strategy for Women’s, Children’s, and Adolescents’ Health.
Disclaimer: All opinions expressed are personal and do not necessarily reflect those of the Independent Accountability Panel for the UN Secretary’s General’s Global Strategy for Women’s, Children’s, and Adolescents’ Health.
Paola Bergallo is an associate professor of law at the Escuela de Derecho, Universidad Torcuato Di Tella, Argentina; an adjunct researcher at the Consejo Nacional de Investigaciones Científicas y Técnicas of Argentina; and a global fellow at the Centre on Law and Social Transformation.
Please address correspondence to Alicia Ely Yamin. Email: aey7@law.georgetown.edu.
Competing interests: None declared.
Copyright: © 2017 Yamin and Bergallo. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- J. Haberkorn, “Trump revives funding ban to groups providing abortion overseas,” Politico (January 23, 2017). Available at http://www.politico.com/story/2017/01/trump-revives-funding-ban-to-groups-promoting-abortion-overseas-234038.
- M. Redden, “Global gag rule reinstated by Trump, curbing NGO abortion services abroad,” The Guardian (January 23, 2017). Available at https://www.theguardian.com/world/2017/jan/23/trump-abortion-gag-rule-international-ngo-funding.
- Donald Trump’s first death-dealing directive from the White House challenged by the Dutch government and others,” International Campaign for Women’s Right to Safe Abortion (Newsletter, January 27, 2017). Available at http://www.safeabortionwomensright.org/donald-trumps-first-death-dealing-directive-from-thewhite-house-challenged-by-the-dutch-government-andothers; L. Basset, “Donald Trump drastically expands ‘Global Gag Rule’ on abortion,” Huffington Post (May15, 2017). Available at http://www.huffingtonpost.com/entry/donald-trump-global-abortion-policy_us_5919bacae4b0031e737f382e; L. Basset, “Donald Trump drastically expands ‘Global Gag Rule’ on abortion,” Huffington Post (May 15, 2017). Available at http://www.huffingtonpost.com/entry/donald-trump-global-abortion-policy_us_5919bacae4b0031e737f382e.
- Whole Women’s Health v. Hellerstedt (2016), 579 US ___.
- UN Economic Commission for Latin America and the Caribbean, Regional Conference on Population and Development in Latin America and the Caribbean, Montevideo Consensus on Population and Development, UN Doc. LC/L.3697 (2013).
- African Commission on Human and Peoples’ Rights, “Launch of the campaign for the decriminalization of abortion in Africa: Women and girls in Africa are counting on us to save their lives!” press release (January 18, 2016). Available at http://www.achpr.org/press/2016/01/d287; African Commission on Human and Peoples’ Rights, Statement by commissioner Lucy Asuagbor during launch of ACHPR campaign for the decriminalization of abortion in Africa (January 18, 2016). Available at http://www.achpr.org/news/2016/01/d207.
- M. Roseman, unpublished talk at Bergen Summer Exchanges, Bergen, Norway (August 23, 2016).
- G. Dancy and C. Fariss, “Rescuing international human rights law from international legalism and its critics,” Human Rights Quarterly 39/1 (2017), pp. 1–36.
- Ley Orgánica sobre el derecho de las mujeres a una vida libre de violencia, Gaceta Oficial No. 40.548 (November 25, 2014) (Venezuela); Ley 26.485 sobre la protección integral para prevenir, sancionar y erradicar la violencia contra las mujeres en los ámbitos en que desarrollen sus relaciones interpersonales (April 1, 2009) (Argentina); Senado de la República, “Senado aprueba sancionar violencia obstétrica,” press release (April 30, 2014). Available at http://comunicacion.senado.gob.mx/index.php/informacion/boletines/12513-senado-aprueba-sancionar-violenciaobstetrica.html.
- World Health Organization, WHO Director-General summarizes the outcome of the Emergency Committee regarding clusters of microcephaly and Guillain-Barré syndrome: WHO statement on the first meeting of the International Health Regulations (2005) Emergency Committee on Zika virus and observed increase in neurological disorders and neonatal malformations (February 1, 2016). Available at http://www.who.int/mediacentre/news/statements/2016/emergency-committee-zika-microcephaly/en; see World Health Organization, Zika virus: Fact sheet (2016). Available at http://www.who.int/mediacentre/factsheets/zika/en.
- D. G. McNeil, Jr., “Delay pregnancy in areas with Zika, W.H.O. suggests,” New York Times (June 9, 2016). Available at https://www.nytimes.com/2016/06/10/health/zika-virus-pregnancy-who.html?_r=0.
- G. Sedgh, S. Singh, and R, Hussain, “Intended and unintended pregnancies worldwide in 2012 and recent trends,” Studies in Family Planning 45/3 (2014), pp. 301–314.
- CLADEM, Sistematización sobre educación de la sexualidad en América Latina (Lima: CLADEM, 2010).
- Center for Reproductive Rights, The world’s abortion laws 2015 (New York: Center for Reproductive Rights, 2015).
- Office of the High Commissioner for Human Rights, Technical guidance on the application of a human rights-based approach to the implementation of policies and programmes to reduce preventable maternal morbidity and mortality, UN Doc. A/HRC/21/22 (2012).
- Ibid.
- Ibid.; Committee on Economic, Social and Cultural Rights, General Comment No. 22, The Right to Sexual and Reproductive Health, UN Doc. E/C. 3/2016/4 (2016); Committee on the Elimination of Discrimination against Women, General Recommendation No. 24, Women and health, UN Doc. CEDAW/C/1991/I/WG.II/WP.2/Rev.1 (1999).
- Office of the High Commissioner for Human Rights (see note 15), para 27.
- Ibid., para 27.
- A. Tamang, M. Puri, S. Masud, et al., “Medical method of abortion using mifepristone and misoprostol can be safely and effectively provided by pharmacy workers trained under harm-reduction framework in Nepal,” Contraception (submitted).
- P. Bourdieux, An outline of a theory of practice (Cambridge: Cambridge University Press, 1977).
- Transforming Our World: The 2030 Agenda for Sustainable Development, G.A. Res. 70/1 (2015).
- A. E. Yamin, “From ideals to tools: Applying human rights to maternal health,” PLoS Medicine 10/11 (2013), p. e1001546.
- See, for example, G. Rubin, “Thinking sex: Notes for a radical theory of the politics of sexuality,” in H. Abelove, M. A. Barale, and D.M Halpern (eds), The lesbian and gay studies reader (New York: Routledge, 1993).