TB in Vulnerable Populations: The Case of an Indigenous Community in the Peruvian Amazon
Camila Gianella, César Ugarte-Gil, Godofredo Caro, Rula Aylas, César Castro, and Claudia Lema
Abstract
This article analyzes the factors associated with vulnerability of the Ashaninka, the most populous indigenous Peruvian Amazonian people, to tuberculosis (TB). By applying a human rights-based analytical framework that assesses public policy against human rights standards and principles, and by offering a step-by-step framework for a full assessment of compliance, it provides evidence of the relationship between the incidence of TB among the Ashaninka and Peru’s poor level of compliance with its human rights obligations. The article argues that one of the main reasons for the historical vulnerability of the Ashaninka to diseases such as TB is a lack of political will on the part of the national government to increase public health spending, ensure that resources reach the most vulnerable population, and adopt and invest in a culturally appropriate health system.
Introduction
There is growing acceptance of the close relationship between tuberculosis (TB) and structural factors such as global and national socioeconomic inequalities, discrimination, poverty, malnutrition, and weaknesses in health systems.1 Recognition of this relationship has led to increasing agreement on the need to include social determinants of TB among the targets of TB programs.
This recognition of the part played by social determinants of health with regard to TB involves identifying states’ responsibilities and the role of other actors in the distribution of the social determinants of TB, as well as the availability of, and access to, care (diagnosis and treatment): that is, making the assertion that TB is a human rights issue. This is a critical feature of the fight against TB, in which emerging approaches to reducing the catastrophic cost of the disease are prioritizing top-down interventions. These, in line with a biomedical tradition, are centered on producing variations such as behavioral changes in individuals with TB by means of conditional cash transfers, leaving aside the implementation of measures for addressing structural forces such as inequity, which not only make certain groups more vulnerable to the disease, but also create barriers to access to health care.2
The adoption of a human rights framework for TB requires a shift in the paradigm, a move away from an approach in which health is defined by experts scientifically and objectively, in isolation from the broader contexts in which people actually live. This is no easy task in the field of infectious diseases such as TB, which has traditionally been understood with reference to a biomedical paradigm, and addressed from the point of view of biological individualism.3 The more communitarian interventions have generally sought to increase TB patients’ autonomy, and to empower them. Many of these interventions have adopted a “rights discourse” at a formal level, and are portrayed as interventions aimed at providing social protection for TB patients (that is, reducing poverty and vulnerability), but they have neither challenged the paradigm of biological individualism nor challenged the structural conditions that make certain groups more vulnerable to TB.
The aim of this article is to provide evidence of the relationship between TB within vulnerable groups and the level of compliance of states with their human rights obligations. By so doing, it seeks to make a contribution to efforts to expand the use of human rights-based analysis in the TB field, and to demonstrate its usefulness and strengths.
In order to assess the current state of compliance, this paper has adopted the methodological framework known as OPERA, developed by the Center for Economic and Social Rights.4 OPERA assesses public policy compared with human rights standards and principles, and offers a step-by-step framework for making a full assessment of compliance: Outcomes, Policy Efforts, Resources, and Assessment. OPERA is based on a multidisciplinary approach that includes input from legal, social sciences, statistics, public policy, and economic fields. OPERA’s analytical approach is in line with the increasing recognition of the fact that health is crucially determined by factors beyond the health sector itself, including the distribution of economic resources, information, and power dynamics at global, national, and local levels.5 The OPERA framework allows these structural factors to be connected with states’ human rights commitments, and demonstrates the relationship between poor health outcomes and shortfalls on the part of states in the fulfilment of their human rights obligations.
The article focuses its analysis on a specific vulnerable group: the Ashaninka, the largest indigenous Peruvian Amazonian people. Owing to the aggressiveness of TB among this population, the Ashaninka are considered to be highly vulnerable to the disease, and consequently are a prioritized group for the purposes of the Peruvian National Tuberculosis Control Program (NTCP).6 However, this high level of vulnerability has mainly been portrayed as a medical phenomenon that excludes an analysis of the disease and its relationship with exclusion structures, or with the level of State compliance with human rights obligations.
Our analysis is based on two principal sources of information. The first is a study commissioned by the Peruvian National Tuberculosis Program, the objective of which was to design a care model for TB prevention and control aimed at the Ashaninka communities. This study was prepared between September 2014 and January 2015 with the participation of two of the authors of this article, Lema and Ugarte-Gil.7 The study collected information from 18 indigenous communities within the catchment area of nine public health clinics in the Pangoa and Río Negro districts of Junín, and included interviews and focus groups with community members and current and former TB patients, and interviews with health care workers. The second source of information was a desk study that included a review of documents and articles produced by the Peruvian Government (including the Ministry of Health, the Peruvian National Tuberculosis Program and the National Multisectoral Coordinator in Health for Global Fund Projects), multilateral agencies such as the World Health Organization (WHO), non-governmental organizations (NGOs), and researchers working on TB and/or with the Ashaninka population in Peru.
Peru: Country background
The distinctive features of Peru include gaps in development and inequities among regions, geographic locations, ethnic groups, and gender. These gaps have persisted despite the country’s economic development. Although Peru is an upper-middle-income country with a gross national income per capita (GNI PPP) of US$11,279.88, a quarter of the population lives in poverty. The notable disparities in the distribution of wealth—income inequality is 48.1—are closely related to gender and ethnic background. It is difficult to establish a single marker of ethnicity in Peru; however, if mother tongue (primary language) is used, it is possible to detect significant differences among ethnic groups. For example, 78% of all indigenous children and adolescents live in poverty, compared with 40% of Spanish-speaking children. Poverty is also more prevalent among rural populations (53%, compared with 16.6% in urban areas), and affects indigenous populations disproportionately (66% of indigenous Peruvian people live in rural areas). Among the indigenous Peruvian population, the Amazonian peoples face a higher incidence of total or extreme poverty (81% and 41%).
As regards the organization of its health system, Peru established its Comprehensive Health Insurance System (Seguro Integral de Salud or SIS) in 2002, in order to “expand health coverage by reducing economic barriers through the elimination of user fees for a package of services.”8 The SIS increased enrolment in health insurance (from 41.7% in 2003 to 54.1% in 2008) and played a significant role in the improvement of certain indicators such as maternal and child mortality, but failed to ensure the provision of integrated health care. In practice, the SIS mostly provided health services for women and children under 18 years old, but did not provide comprehensive care to the adult population as a whole.9 Consequently, a new policy, known as Universal Health Insurance (Aseguramiento Universal de Salud or AUS) was approved in 2009 with the aim of “providing universal health coverage to the entire Peruvian population.”10 The AUS contemplates the provision of a basket of services (Plan Esencial de Aseguramiento en Salud or PEAS) to the entire Peruvian population. There are three mechanisms for enrollment in the AUS: through insurance contributions (payroll deductions and private payments), semi-contributions (a combination of private and public contributions to cover informal and small business workers), and subsidized insurance for the poor (covered by public funds, and intended to replace the SIS). There has been little progress in the implementation of the AUS to date, however: according to some scholars, the SIS’s resources are not sufficient to cover the PEAS.11 As resources allocated to health sector remain low, it is not clear how the costs of the PEAS for the worst-off will be covered.
Information on health insurance coverage among indigenous peoples is not available. The reports on health insurance coverage prepared by the authorities only identify the percentage of the population covered by regions and provinces (totals) and type of insurance, and do not offer data disaggregated by ethnicity.
The Ministry of Health (MoH) is in charge of TB prevention and treatment through the National Tuberculosis Program (NTP). In principle, the NTP has been available to the entire population through the public health service network for many years at no direct cost. It provides a wide range of services, including diagnostic tests, HIV testing, and TB treatment (under the Directly Observed Treatment, Short Courses (DOTS) scheme, which was implemented nationwide in 1991).
The indigenous Amazonian people of Peru were selected for this research because of a high incidence of TB and the aggressiveness of the disease in this population group. Oil exploration and logging in indigenous Amazon territories have led to an influx of workers who have exposed the indigenous people to new diseases. When TB arrives in a population that has not been previously exposed to it, such as the indigenous Amazonian people, it develops more aggressively, with a high percentage of extra-pulmonary TB accompanied by a rapid spread within the communities.12
This study focuses on the Ashaninka from the Junín region. The Ashaninka make up the largest Peruvian Amazonian indigenous group, and 54.74% of them live in Junín.13 In addition, according to data gathered from Peruvian indigenous peoples (not in the form of a regular MoH report), the Ashaninka who have settled in Junín have the highest prevalence of TB.14
Like other Peruvian indigenous Amazonian peoples, the Ashaninka are subject to social exclusion, and have lived through a history of mistreatment and disproportionate violence. They suffered during the internal armed conflict between 1980 and 2000 to an undue degree: 6,000 Ashaninka were murdered, 10,000 were forcibly displaced, 5,000 were kidnapped and held prisoner for years, and dozens of their communities disappeared.15 Because their territories are so rich in natural resources such as wood, oil, minerals, and water, the Peruvian Amazonian indigenous peoples, including the Ashaninka, are currently facing new struggles with the national government, many of which are related to a refusal on the part of the national authorities to recognize indigenous peoples’ right to be consulted prior to extractive activities being developed in their ancestral territory. Consequently, land property, and title to land, are critical and highly sensitive issues in Peru. The Peruvian Amazon comprises 60.9% of the national territory, and indigenous peoples have 27.1% of the Amazon under ownership or assignment or in their possession but despite this many hundreds of indigenous communities lack any legal title, which places them in a vulnerable situation.16
The vulnerability of indigenous communities has been aggravated by the pro-private investment policies adopted by Peru, of which one example is Law 30230, passed in July 2014, which weakens environmental safeguards to promote private investment. Law 30230 also increases the vulnerability of, and pressures on, indigenous territories by granting the central government powers to allocate land rights for large investment projects (including mining, forestry, and agribusiness), regardless of the land’s current or future use. Law 30230 represents a major setback for the country’s policies on climate change, and was approved without the technical approval of the Ministry of Environment.
The Junín Ashaninka have not been isolated from these struggles: gas exploration in the Ashaninka territory in Junín without prior consultation has triggered major protests in recent years.17 They also have an ongoing legal struggle with the national government relating to construction of the Pakitzapango hydroelectric dam, which would flood much of the Ene River valley, thereby forcing the Ashaninka to migrate.18
Step 1 – Outcomes: Assessing the level of enjoyment of rights
The outcomes step assesses the enjoyment of rights, applying the human rights standards of minimum core obligations, non-discrimination, and progressive realization. This analysis, mainly based on descriptive data, allows measuring the extent of the realization of the right(s) under review in the country. The application of these standards is not arbitrary; the “minimum core obligation standard” measures the aggregate levels of rights enjoyment, the standard of “non-discrimination” assesses disparities in rights enjoyment, while the standard of “progressive realization” measures changes and progress over time on the rights enjoyment.19
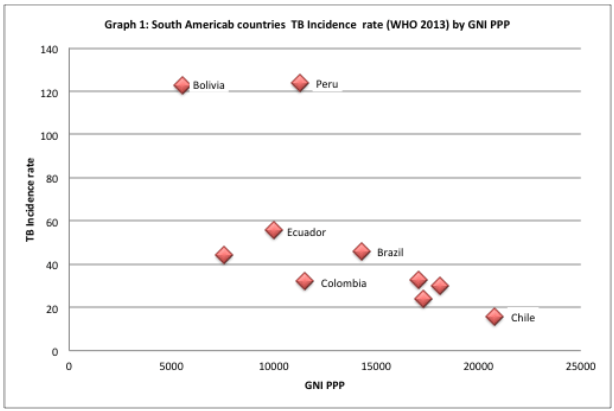
Peru is home to 3.1% of the population of the Americas, and yet it reports 13.6% of TB cases (new and relapses) and 41% of confirmed cases of multidrug-resistant TB (MDR-TB) in Latin America.20 Its incidence and prevalence exceed both regional (121 per 100,000 inhabitants and 95 per 100,000 inhabitants respectively, against a regional incidence of 29 per 100,000 and prevalence of 40 per 100,000) and world levels.21 If Peru is compared with other Latin American countries with similar or lower GDPs, its poor performance becomes evident: all Latin American countries with similar or lower GDPs have lower rates of incidence of TB (see Figure 1). Peru’s high incidence contradicts what has been suggested by some scholars, such as Janssens and Rieder who have found a relationship between TB incidence rates and national income.22 This result suggests that in the case of Peru, national income is not the principal reason behind the high rates of TB.
As regards the principle of non-discrimination, there are no reliable data on the prevalence of the disease by ethnicity; these data are not collected, because the form designed and used by the Peruvian National Tuberculosis Program (NTP) has no fields relating to ethnicity.
In relation to the progressive realization of rights, it should be noted that Peru was a pioneer on implementing the Directly Observed Treatment, Short Courses (DOTS) program at a national level.23 Implementation of the DOTS, which is free of charge nationally, has produced a number of positive results: there has been a sustained decrease in the number of cases of sensitive TB (which form the majority of cases) at a national level, and the NTP has maintained the percentage of cured patients over 80% for many years.24 The numbers of cases of MDR-TB have continued to grow, however, and the emergence of extensively drug-resistant tuberculosis (XDR-TB) in Peru constitutes a threat to the country.25 Besides, although Peru has declared that MDG 6C on TB control has been achieved, reporting a national incidence rate of 90.3 per 100,000 inhabitants in 2013, in the areas in which 60% of cases of sensitive TB are concentrated, the incidence has remained higher than that expected by the MDG: over 96 cases per 100,000 inhabitants.
The province of Satipo reported by 2013 a TB incidence of 54 cases per 100,000 inhabitants; however, in the districts covered by the NTP study, the reported incidence is higher than the provincial one: Pangoa reported the same year an incidence of 80 and Rio Negro an incidence of 75. Despite this, as has been mentioned, in districts with a high concentration of indigenous people, the available information does not allow an estimate of how many of the people with newly diagnosed TB are Ashaninka.
Step 2 – Policy efforts
This step combines qualitative and quantitative indicators and aims to assess the commitments and efforts made by the state to realize the right(s) under review. As a second step, OPERA examines three principles of human rights: i) the obligation to take steps; ii) acceptability, availability, affordability, adaptability, and quality (the AAAAQ criteria); and iii) participation, transparency, accountability, and the right to a remedy.
Determination of the obligation to take steps requires an analysis of the legal commitments made by the State. For this case study, we analyze the legal commitments adopted by Peru on the right to health, and the rights of indigenous peoples. This includes Peru’s Constitution and its domestic legislation, as well as international treaties to which it is a party. It should be noted that case law from the Peruvian Constitutional Court has established that international treaties have constitutional status.27 In addition, the fourth Final and Transitory Provision (Disposición Final y Transitoria Cuarta) of 2004 clarifies that “the norms relating to rights and liberties recognized in the Constitution are to be interpreted in accordance with the Universal Declaration of Human Rights and the human rights treaties and agreements that have been ratified by Peru.”28
At a UN human rights system level, the International Covenant on Economic, Social and Cultural Rights (ICESCR) is considered to be the central instrument for protection of the right to health. This covenant recognizes “the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.” Other key international treaties that recognize the right to health to which Peru is a party are the 1965 International Convention on the Elimination of All Forms of Racial Discrimination, the Convention on the Elimination of All Forms of Discrimination against Women, the Convention on the Rights of the Child, and the Convention on the Rights of Persons with Disabilities.
At a regional level, the American Declaration of the Rights and Duties of Man references the right to health in Article 11, and the Additional Protocol to the American Convention on Human Rights on Matters Relating to Economic, Social and Cultural Rights (Protocol of San Salvador), to which Peru is also a party, specifically includes the right to health in Article 10.
As regards the right of indigenous people to have access to health services, Article 25 of International Labour Organization Convention 169 concerning Indigenous and Tribal Peoples in Independent Countries (ILO Convention 169) declares that states have an obligation to make adequate health services available to indigenous peoples, considering their social, economic, and geographical situation and their culture. The convention states that social security schemes must be extended progressively to indigenous peoples without discrimination, and that health services should be organized at a community level as far as possible, with the participation of indigenous peoples in planning and administrating health services (Articles 24 and 25.2 respectively). Participation by, and consultation with, indigenous peoples on measures taken by the State that may affect them are the foundations of ILO Convention 169.
As far as domestic legislation is concerned, the 1993 Peruvian Constitution recognizes the right to health (Article 7), as well as the right to ethnic and cultural identity (Article 2). It also establishes the State’s obligation to respect the cultural identity of indigenous communities (Article 89). In addition, the Peruvian General Health Law recognizes the right to health as an element of the public interest and public responsibility of the State. The same law states that the management and regulation of actions to prevent, control, and eradicate communicable diseases throughout the country fall within the responsibilities of the national health authority. In 2014, the Law for TB Control and Prevention (Law 30287) was passed, and among the rights of people infected with TB includes the right to receive complete treatment (prevention, diagnosis, treatment rehabilitation, and where required, specialized care according to the national TB Guidelines). Law 30287 provides details on how health workers and prison inmates who become infected with TB must be treated, and provides for measures to prevent discrimination and mistreatment; however, it does not mention indigenous peoples or the need to provide culturally appropriate health care.
The 2013 Peruvian National TB Guidelines do, however, list the indigenous Amazonian peoples as a TB-vulnerable group, and recognize the need to create synergies between the indigenous people’s health systems and the Western system (a biomedical approach), as well as the State’s mandate to ensure the provision of TB care applying an intercultural approach towards indigenous peoples. According to the 2013 guidelines, these activities must be coordinated with the National Strategy of Indigenous People, but in practice this has not been implemented.
In October 2014, with the aim of increasing coverage of state social programs among indigenous Amazonian peoples, the Peruvian government issued a package of executive decrees, which required, inter alia, all inhabitants of indigenous Amazonian communities to be classified as a population living in extreme poverty, and consequently as beneficiaries of social programs such as free public health insurance (SIS). Prior to this decree, the inhabitants of indigenous Amazonian communities faced extensive administrative barriers when attempting to demonstrate that they were poor, and consequently to have access to social programs financed by the central government.
In short, Peru has committed to protecting and guaranteeing its indigenous populations’ right to health. In order to analyze to what extent these commitments are reflected in actual policies, we have applied the AAAAQ criteria.
Acceptability
Cultural acceptability is a core issue in health programs, especially among populations that have been historically discriminated against based on their ethnic origins and cultural identities. The Peruvian authorities have recognized the need to adopt an intercultural health approach and its importance.29 One main characteristic of such an approach is that it is based on mutual respect for and equal recognition of indigenous and Western health systems.30 Health care provided by the public health network must therefore reflect this dialogue and the mutual recognition and respect between the different health systems.
From an Ashaninka perspective, health represents a balance between a person’s internal and external factors. This balance guarantees individual and collective health. Throughout their history, the Ashaninka have developed practices that allow them to remain healthy and to strengthen the health of their families. In general, these practices relate to compliance with a series of rules that govern interaction between the genders and with the community and the natural environment that surrounds them. They also include the consumption of a number of medicinal plants that allow them to maintain their physical strength and prevent disease.
The Ashaninka believe that their traditional health system can be trusted, but they also accept that in the case of some diseases, such as TB, health centers (the Western approach) are also a reliable source of healing. Their general practice is first to seek treatment within their own traditional healing system, and then to go to a health center. In the case of TB, they look for healing from the sheripiari (traditional healer) and the shimpokantantantsiro (the steamer, who is female). It should be noted that the Ashaninka do not abandon their traditional medicine when they go to a Western health center: they may continue consuming herbs and fruit recommended by their traditional healers in association with the treatment provided by the health center; this shows that as far as they are concerned, use of the synergies between these two systems is common practice.
An intercultural health system must engage in a dialogue with these concepts, knowledge, and practices. Generally speaking, health workers believe that the Ashaninka perception and understanding of the disease is wrong, and workers in charge of TB control and prevention activities among Ashaninka communities in Junín have not promoted dialogue or exchanges with the Ashaninka healers.
This lack of recognition of the value of the Ashaninka healing system is mirrored in the National TB Guidelines, which have adopted a single standardized approach to TB treatment and control that does not include the Ashaninka understanding of the disease or their knowledge and practices. The TB treatment guidelines used for the Ashaninka are the same standardized versions that are applied at a national level; very little has been done to systematize the Ashaninka’s health system, to introduce their knowledge into their health services network, or to develop guidelines that take this knowledge and these practices into consideration. The NTP has only recently commissioned studies to design a model of care for the Ashaninka, and they have yet to be implemented.
The only initiative developed for working with members of the community relates to the work done by community health workers, but they are used mainly as translators, as channels of communication for transmitting Western knowledge to the communities in their own language.
Availability
In addition to being acceptable, the services must be available. The Ombuds Office has reported that health facilities in the Peruvian Amazon are staffed by poorly trained health workers, and do not have transport facilities for patients, nor adequate cold chain systems for the transport and storage of vaccines.31
According to Peruvian law, TB diagnosis and treatment must be available at public health facilities free of charge for all who need it. Active case detection is a core element of TB control activities, but due to a lack of resources (such as economic resources to cover transport costs), health workers do not have the capacity to organize activities within the communities. One of the problems in isolated rural settings such as the Ashaninka communities is the multiple roles of the health workers, especially in situations where they need to cover a large geographical area for health campaigns, such as vaccinations and disease screening.
Poor availability of timely diagnosis is also a major problem in Ashaninka communities. Not all the health centers in the area included in the study have the capacity to take and prepare samples and transport them to the reference laboratory on time. In addition, the reference laboratories are not always able to return the results in a timely fashion. The health workers interviewed during the study commissioned by the NTP reported that sputum samples from the communities located along the river are collected once a month, regardless of when the samples are taken, which means that some samples can be awaiting analysis for almost a month. During this protracted waiting time, the samples become useless for diagnosis purposes, which raises serious doubts about the quality of the diagnoses. Because the health workers have to wait almost a month to receive the results, this prolonged waiting time has a negative impact on the quality of the service.
Accessibility
The geographic accessibility of health facilities is another major problem the Ashaninka face in Peru. For example, primary health clinics (PHCs) such as those included in this study may be four or more hours away on foot. This represents a significant challenge for a DOTS TB strategy that requires daily visits to health clinics during the intensive phase.
Access to information on TB and its management and treatment and the quality of this information have been identified as a major gap in the fight against TB in Peru. Misinformation has been associated with poor treatment compliance (intermittent assumption of treatments may result in treatment resistance) and treatment default among TB patients.32 Although most of these studies have been performed in urban areas, mainly in Lima, the evidence suggests that information also represents a major weakness of the NTB among the Ashaninka. In general, health education and communication materials available in the province are not appropriate for indigenous people in terms of the language (in Spanish, rather than Ashaninka) and illustrations. Both the interviews and observations in the health clinics indicated that most of the materials are targeted to the urban population from the coast. Efforts to produce appropriate TB education and information for Ashaninka communities have been made with the support of the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), but distribution and actual use of the information was not observed in Satipo. Besides the fact that the materials are in Spanish, the health workers often do not speak Ashaninka: in fact, at the health facilities included in the study commissioned by the NTP, there were no Ashaninka-speaking health workers. This means that in the network of health care facilities (which consists mainly of PHCs) covering a population of approximately 21,072 inhabitants, the majority of whom are Ashaninka, it is not possible to provide care in the language of the majority population.33
Besides the lack of availability of information in Ashaninka, users have reported mistreatment by health care workers. In the interviews, they refer to situations in which health care workers shout at them for not being on time, or where the information provided by health workers is unclear. These reports of health care workers mistreating the Ashaninka match previous research carried out on other services (such as maternal care) at public health facilities in the same area.34
Affordability
Affordability is another core element of access to health care, and the Ashaninka living in communities in the Peruvian Amazon are entitled to free health insurance because of their poverty status; however, the interviews taken from Ashaninka from Junín show that is not clear to them that drugs and tests must be provided without charge. In addition, transportation costs to the health facility or to a health center that offers more services (such as a doctor or chest X-rays) are not covered. The population also needs to invest its own time, which is a valuable resource for the Ashaninka, who need to use it to create income, work on their land, or perform other activities to ensure that their families are fed. For many Ashaninka, access to health care facilities means a major investment (the time invested in treatment has been identified as an indirect cost of TB treatment).35
Human rights principles
As far as the principles of participation, transparency, accountability, and the right to a remedy is concerned, the data gathered reveals grave deficiencies in the design and implementation of the TB program. As pointed out above, the National TB Program has been designed for an urban population living in the major cities on the coast. Indigenous populations were not involved in the design of the guidelines, prevention activities, or informational materials. This lack of an effective participation mechanism is a common factor in the design and implementation of policies for the indigenous populations of Peru. At a regional level, the methodology for the preparation of the Regional Concerted Health Plan 2013-2021 did not include any mechanism to avoid neglecting the health needs of minorities (by size), or groups with a right to special protection, such as the indigenous Amazonian communities.36 In a region where the Andean population is in a majority, the process for the elaboration of the Regional Concerted Health Plan ended up by making the interventions that had been prioritized by the majority, and, as might be expected, the Plan’s outcome impact indicators do not include indicators on the health of indigenous people (including the indigenous Amazonian people). Finally, the Plan does not include any representatives of indigenous communities among its signatories.
Step 3 – Resources: Assessing the use and generation of adequate resources
The ICESCR’s recognition that full realization of ESC rights can only be achieved gradually—as resources permit—is an important qualifier of the obligation to take steps. Nevertheless, states must show that the steps they have taken—the programs, plans, and services assessed above—have benefited from the “maximum available resources”. The third step of the OPERA framework focuses on the analysis of the resources (budgetary and other fiscal resources) allocated by the state to meeting its human rights commitments.
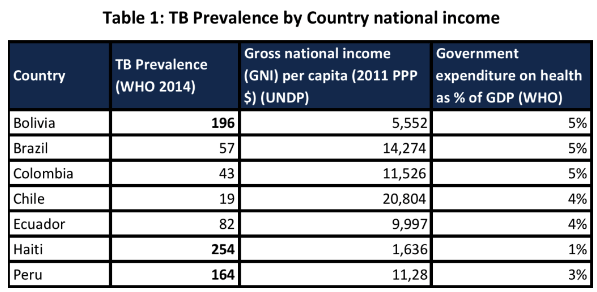
While the country has experienced favourable economic growth, the percentage of GDP allocated to the health sector has not increased significantly, and is below that allocated by other Latin American countries with a similar or lower GDP (see Table 1).
It should be noted that the Peruvian NTP has received significant financial support from the Global Fund: US$72,223,009, compared with the US$21,348,359 received by Brazil since the creation of the fund. The amount received from the Global Fund indicates that although Peru is an upper middle-income country, the NTP is still highly dependent on external funding. The financial resources received from Round 8 of the Global Fund have been used to cover the expenses of regular national communication campaigns, to strengthen laboratory networks, and to universalize MDR-TB treatment. In a country like Peru, with its historically high prevalence of TB, and with the highest incidence of MDR-TB in the region (and one of highest in the world), it would be expected that the annual public budget would include the allocation of resources to cover regular TB information campaigns and the strengthening of national TB response activities. This low investment in TB-related activities reflects a national trend of poor performance on investment in welfare and social programs.37
Besides, the health authorities in Junín and Satipo have not prioritized TB activities among those marked for capitation payments: a lump sum paid to the region or the district by the national government against the accomplishment of pre-defined goals. These goals and targets are used to evaluate the performance of the health services and health workers. Consequently, the activities included in these agreements are prioritized. By excluding TB activities from these agreements, TB prevention and control activities are put at the bottom of the list of the priorities of health workers.
Step 4 – Assessment
The fourth and final step of the OPERA framework makes a final assessment of a state’s compliance with its obligation to fulfil the rights under review. The overall assessment raises concerns and questions regarding Peru’s willingness to fulfil its human rights obligations. The signature and formal legal recognition of indigenous rights and the right to health have not granted access to quality health services to TB patients or the Ashaninka population.
The Peruvian government has committed to improving access to health care for the indigenous population of the Amazon region, with enrollment in the SIS being one of the major strategies. August 2015 reports on coverage from the SIS, however, do not show an increase of the coverage within Satipo since November 2014. Even if such an increase was present, it would not necessarily denote an increase in respect for the knowledge of the indigenous population, or for the implementation of an intercultural health system.
It is to be hoped that this case study will also show the limitations of “blind use” of national health indicators. As this study shows, the national data reported to assess the performance of the Peruvian NTP have not been sensitive to the challenges faced by historically excluded, vulnerable, or minority populations. Moreover, the pressure for improved health outcomes at a national level may lead to the health needs of minority groups being ignored. Peru’s compliance regarding the protection of the rights of the indigenous Amazonian population, including their rights to health, cannot be assessed without data, and one of the central issues is therefore the lack of a national information system with the ability to report on indigenous people’s health.
Conclusion
Our analysis of TB in the Ashaninka population of Junín shows that despite the formal commitments made by Peru, the Ashaninka’s right to health in the sense required by national and international human rights instruments has not been respected, in that protection of this population’s right to health has not been achieved.
The shortcomings we have described in the information system and access to health care (including information), as well as the low levels of investment in the health sector, provide evidence of the structural factors behind the high level of vulnerability of the Ashaninka to TB, and illustrate the close association between TB and human rights. These results agree with previous research in requesting a NTP with a comprehensive approach that goes beyond the formal provision of medicines and development of new diagnostic tools, including social determinants of health.38 One of the most salient features of the application of human rights analysis frameworks such as OPERA, however, is an explicit demand for a shift in the paradigm of addressing TB from a biomedical tradition centered on the individual to one that is more focused on interventions to address structural forces.
Research performed in Peru has already shown that the weakness of the health system, including a lack of access to timely diagnosis, has a major negative impact on TB treatment outcomes.39 This evidence has prompted the development of interventions that adhere to a biomedical tradition, and are therefore almost exclusively focused on the need to change the behavior of individuals with TB, and neglect to address critical conditions such as low investment in the health sector and poverty.40 By demonstrating the central role played by political decisions in the provision of TB care (through the enactment of policies or the allocation of resources), the analysis undertaken in this paper seeks a change in focus to one that includes the state and the need to make the state accountable for complying with its human rights obligations.
Camila Gianella, PhD, is researcher at Chr. Michelsen Institute in Bergen, Norway, and post-doc researcher at the Department of Comparative Politics, University of Bergen, Norway.
César Ugarte-Gil is Consultant at Salud Sin Limites Peru, and Research Associate at Instituto de Medicina Tropical Alexander von Humboldt, Universidad Peruana Cayetano Heredia, Lima Peru; and PhD student at Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Rula Aylas, is member of the technical team at Indigenous Health Directorade at the Ministry of Health, Lima, Perú.
César Castro, is lecturer at School of Nursing Universidad Peruana Los Andes, Huancayo, Perú.
Claudia Lema, is Executive Director at Salud Sin Limites Peru, Lima, Peru.
Godofredo Caro, is TB consultant medical doctor at Mantaro Health Network, Junin Health Directorate, Junín, Perú.
Corresponding author: Camila Gianella. Email: Camila.gianella@cmi.no
Competing interests: None declared.
Copyright © 2016 Gianella, Ugarte-Gil, Caro, Aylas, Castro, and Lema. This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- J.R. Hargreaves, D. Boccia, C.A. Evans, M. Adato, M. Petticrew, J.D.H. Porter. “The Social Determinants of Tuberculosis: From Evidence to Action,” American Journal of Public Health 101/4 (2011), pp. 654-62.
- A.M. Medeiros da FonsecaI, A.L. d’Ávila Viana. “Direito à saúde, atenção básica e transferências condicionadas de renda na América Latina.” Ciênc saúde coletiva 12/6 (2007); J. Jenson, N. Nagels. “Social Policy Instruments in Motion. Conditional Cash Transfers from Mexico to Peru.” ICPP. Milan (2015).
- A.E. Yamin. “Will We Take Suffering Seriously? Reflections on What Applying a Human Rights Framework to Health Means and Why We Should Care.” Health and Human Rights 10/1 (2008), pp. 45-63.
- Center for Economic and Social Rights. “The OPERA Framework Assessing compliance with the obligation to fulfill economic, social and cultural rights,” Center for Economic and Social Rights (2012).
- Commission on Social Determinants of Health. “Closing the gap in a generation: Health equity through action on the social determinants of health”. Geneva: World Health Organization (2008).
- Ministerio de Salud. “Norma Técnica para la Atención Integral de las Personas Afectadas por Tuberculosis.” Lima: Ministerio de Salud (2013).
- Pathfinder International, Consorcio Socios en Salud Sucursal Perú, Proceso Social. “Propuesta de modelo de atención con enfoque intercultural en la estrategia de prevención y control de TB en comunidades asháninkas.” Pathfinder International, Consorcio Socios en Salud Sucursal Perú, Proceso Social. Lima (2015).
- P. Francke. “Peru´s Comprehensive Health Insurance and New Challenges for Universal Coverage”. Washington DC: The World Bank (2013).
- M. Petrera, M. Valdivia, E. Jimenez, G Almeida. “Equity in health and health care in Peru, 2004-2008”. Revista Panaméricana de Salud Pública 33/2 (2013) pp. 131-6.
- Ibid.
- R. Bitrán, A. Burgos. “Experiencias Latinoamericanas en la Búsqueda de la Cobertura Universal en Salud”. USAID (2012).
- Ministerio de Salud. “Plan Estratégico Multisectorial de la Respuesta Nacional a la Tuberculosis en el Perú 2010-2019”. Lima, Ministerio de Salud (2010).
- Fundación Cayetano Heredia. “Estudio de vulnerabilidades y factores de riesgo asociados a la tuberculosis en comunidades indígenas asháninkas. Informe Final.” Lima, Socios en Salud (2011).
- Instituto Nacional de Estadística e Informática. “II Censo de comunidades amazónicas” Lima, INEI (2007).
- Comisión de la Verdad y Reconciliación. “Los pueblos indígenas y el caso de los ashaninkas.” Lima: Informe Final Comisión de la Verdad y Reconciliación, 2.8. ( 2003)
- M. Benavides. “Amazonía peruana: el choque de dos visiones de desarrollo. La protesta indígena del 2008 y 2009 frente a los derechos legislativos que afectaban sus territorios.” Lima: Instituto del Bien Común, (2010).
- D. Pereira. “¿Qué está pasando en Pichanaki? Esto es lo que debes saber del conflicto que podría convertirse en otro Baguazo.” Available at http://utero.pe/2015/02/11/que-esta-pasando-en-pichanaki-esto-es-lo-debes-saber-sobre-el-conflicto-que-podria-convertirse-en-otro-baguazo/
- Central Ashaninka del Río Ene, Centro Amazónico de Antropología y Aplicación Práctica. “Situación de vulnerabilidad del pueblo ashaninka relacionadas con actividades energéticas.” Perú (report presented at the Comisión Interamericana de Derechos Humanos, Peru, 138 period of sessions 2010).
- Center for Economic and Social Rights (see note 4.)
- World Health Organization.”Global tuberculosis report” Geneva: World Health Organization (2014).
- Ibid.
- J-P, Janssens, H.L. Rieder. “An ecological analysis of incidence of tuberculosis and per capita gross domestic product.” European Respiratory Journal 35/5 (2008) pp. 1415-6.
- P.G. Suárez, C.J. Watt, E. Alarcón, et al. “The Dynamics of Tuberculosis in Response to 10 Years of Intensive Control Effort in Peru.” The Journal of Infectious Diseases 184/4 (2001) pp. 473-8.
- A. Alarcón. “Situación de la Tuberculosis en el Perú y política nacional para su control. Arequipa, Peru: (Presentation at the technical meeting “Evaluación y Análisis de Indicadores Epidemiológicos y Operacionales Año 2013 en Relación al Presupuesto por Resultados”, 2014).
- L. Asencios, N. Quispe, A. Mendoza-Ticona, et al. “Vigilancia nacional de la resistencia a medicamentos antituberculosos, Perú 2005-2006.” Revista Peruana de Medicina Experimental y Salud Pública 26/3 (2009).
- Alarcón (see note 24.)
- R. Villanueva. “Derecho a la salud, perspectiva de género y multiculturalismo.” Lima: Palestra (2009).
- Congreso de la República. Disposiciones Finales y Transitorias. Available at http://www4.congreso.gob.pe/accesible/constitucion/disposicionesfinales.htm (November 17, 2004.)
- Ministerio de Salud. “Norma Técnica para la Transversalización de los Enfoques de Derechos Humanos, Equidad de Género e Interculturalidad en Salud.” Lima: Resolución Ministerial 638-2006/MINSA (2006).
- M.C. Tori. “Intercultural Health Practices: Towards an Equal Recognition Between Indigenous Medicine and Biomedicine? A Case Study from Chile. Health Care Anal 2012 20 (2012) pp. 31–49.
- Defensoría del Pueblo. “La Salud de las Comunidades Nativas: Un reto para el Estado.” Lima: Defensoría del Pueblo (2011).
- D.R. Culquia, C.V. Munayco, C.G. Grijalvac, et al. “Factors Associated With the Non-completion of Conventional Anti-Tuberculosis Treatment in Peru.” Archivos de Bronconeumología 48/5 (2012).
- Dirección Regional de Salud de Junín. “Población Oficial Estimada por Edades Puntuales y Grupos Quinquenales Según Redes, Provincias, Distritos y Establecimientos de Salud DIRESA Junín 2014”. Dirección Regional de Salud de Junín – Oficina de Estadística e Informática (2014).
- Salud Sin Limites. “Madre Nativa: experiencias acerca de la salud materna en las comunidades ashaninkas y nomatziguengas”. Lima: Salud Sin Limites (2008).
- T. Wingfield, D. Boccia, M.A. Tovar, et al. “Defining Catastrophic Cost and Comparing Their Importance for Adverse Tuberculosis Outcome with Multi-Drug Resistance: A Prospective Cohort Study,” Peru. Plos Medicine (2014); 11/7 e1001675.
- Gobierno Regional de Junín, Dirección Regional de Salud de Junín. “Plan Regional Concertado de Salud de Junín 2013 – 2021.” Huancayo, Peru: Dirección Regional de Salud de Junín (2012).
- American Quarterly. “Americas Quarterly Social Inclusion Index 2015.” Available at http://www.americasquarterly.org/charticles/social-inclusion-index-2015/social_inclusion_index_2015-english.pdf.
- C. Rocha, R. Montoya, K. Zevallos, et al. “The Innovative Socio-economic Interventions Against Tuberculosis (ISIAT) project: an operational assessment.” International Journal of Lung Disease (2011) 15 (Suppl 2): S50–S7.
- S.L. Bailey, M.H. Roper, M. Huayta, et al. “Missed opportunities for tuberculosis diagnosis.” International Journal of Lung Disease 15/2 (2011) pp. 205-10. (See also notes 32 and 35.)
- Wingfield T, Boccia D, Tovar M, A, et al. “Designing and implementing a socieconomic intervention to enhace TB control: operational evidence from the CRESIPT project in Peru.” BMC Public Health 2015; 15 p.810.