Indigenous Child Health in Brazil: The Evaluation of Impacts as a Human Rights Issue
Anna R. Coates, Sandra del Pino Marchito, and Bernardino Vitoy
Health and Human Rights 18/1
Published June 2016
Abstract
Improving the health status of indigenous children is a long-standing challenge. Several United Nations committees have identified the health of indigenous peoples as a human rights concern. Addressing the health of indigenous children cannot be separated from their social, cultural, and historic contexts, and any related health program must offer culturally appropriate services and a community perspective broad enough to address the needs of children and the local worlds in which they live. Evaluations of programs must, therefore, address process as well as impacts. This paper assesses interventions addressing indigenous children’s health in Brazil, ranging from those explicitly targeting indigenous children’s health, such as the targeted immunization program for indigenous peoples, as well as more generalized programs, including a focus upon indigenous children, such as the Integrated Management of Childhood Illness. The paper discusses the tensions and complexities of ethnically targeted health interventions as well as the conceptual and methodological challenge of measuring the processes employed and their impact. The lessons learned, especially the need for countries to more systematically collect data and evaluate impacts using ethnicity as an analytical category, are drawn out with respect to ensuring human rights for all within health sector responses.
Introduction
Indigenous children throughout the world suffer one of the most severe burdens of ill health of any population group, clearly reflecting the results of the intersection of multiple forms of inequalities. Across the globe, there are significant health disparities between indigenous and non-indigenous populations, ranging from infectious diseases such as HIV/AIDS, malaria, and tuberculosis (TB) to cardiovascular disease, diabetes, cancer, and respiratory diseases. Many of the most widespread causes of mortality among indigenous children are preventable, such as malnutrition, diarrhea, parasitic infections, and TB. In Latin America, indigenous infant mortality rates are consistently higher than those of the general population, ranging from 1.11 times higher in Chile to 3.09 times higher than the general population in Panama.1
This situation is an evident violation of the right to health, as expressed in the constitution of the World Health Organization:
The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.
Several human rights treaty bodies have addressed the situation of indigenous children and their right not to be discriminated against, revealing a global-level awareness of their specific situation of vulnerability and the requirement for special measures in order that such children fully enjoy their rights.2 However, such bodies contemplate the right to health only minimally with respect to indigenous children; indeed, the committee on the CRC only covers it in specific terms in its General Comment No. 11: Indigenous Children and Their Rights Under the Convention.3
Despite this mixed picture, some countries, among them notably Brazil, have taken up the issue as a political priority, not only acceding to most international conventions but also putting into place dedicated institutional structures, policies, and programs that aim to ensure their implementation, as well as monitor their impact in terms of achieving the right to health for indigenous children. The explicit targeting of health interventions towards indigenous children on the basis of their ethnic identity is, however, not without tensions from a rights perspective. Similarly, the measurement of the impact of these interventions implies a degree of complexity from the same rights lens, as well as in terms of the conceptual and methodological challenges this measurement implies, and in terms of the need to take into account the rights issues associated with the process of achieving results.
This paper is based upon a comprehensive review of secondary grey literature regarding the international framework that addresses the right to health of indigenous peoples in general and, specifically, of indigenous children. Reports submitted by the Government of Brazil to those relevant international human rights treaties that address the right to indigenous child health have also been considered and reviewed. The research also included a revision of policy documentation and other reports, laws, policies, and programs related to the health of indigenous children in Brazil. Relevant reports from human rights committees with specific recommendations to the country have also been taken into account.4
Normative frameworks addressing indigenous child health
Global normative frameworks
Of clearest global significance in relation to indigenous people’s rights generally is the 2007 adoption of the United Nations General Assembly Declaration on the Rights of Indigenous Peoples, which includes specific reference to the rights of indigenous children in a number of areas. However, despite its significance at a global level and as a policy reference at the country level, it is not a binding normative framework, and so does not serve as a mandate for UN Member States’ action and accountability.
The most relevant binding normative frameworks that directly or indirectly address the rights of indigenous children include the Convention on the Elimination of All Forms of Racial Discrimination (1965) (CERD), and especially the Committee’s General Recommendation No. 23, Indigenous Peoples (1997); the Convention on the Elimination of All Forms of Discrimination against Women (1979) (CEDAW); the International Covenant on Civil and Political Rights (1966); the International Covenant on Economic, Social and Cultural Rights (1966); and, importantly, the International Labour Organization Convention (ILO) No. 169 concerning Indigenous and Tribal Peoples in Independent Countries (1989). The latter convention regulates the rights of indigenous peoples, including health, and contains provisions that specifically highlight the rights of indigenous children regarding education.5
Of special importance is the Convention on the Rights of the Child (1990) (CRC), which offers a guide to States parties on their obligations towards children and their health, including indigenous children. Among other relevant articles, Article 24 of the CRC addresses the specific right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. It includes the obligations of States parties to take appropriate measures to: (a) diminish infant and child mortality; (b) ensure the provision of necessary medical assistance and health care to all children with emphasis on primary health care; (c) combat disease and malnutrition. The CRC’s provisions should be interpreted in line with other recommendations, which request States parties to work closely with indigenous peoples and organizations to seek consensus on development strategies, policies, and projects aimed at implementing children’s rights, and to especially address their health indicators, to ensure equal access for indigenous children to culturally appropriate health services.6
Regional normative frameworks
Of specific relevance to health, member states of the Pan American Health Organization (PAHO) have paid specific attention to indigenous peoples’ rights to health. In 1993, PAHO’s 37th Directing Council passed Resolution CD37.R5: Health of the Indigenous Peoples of the Americas, which urged the formulation of policies and strategies geared towards specific indigenous populations and was aimed at ensuring their greater access to high-quality health services and care. This commitment was reiterated in 1997, with the approval of Resolution CD40.R6.7 In 2006, Resolution CD47.R18: Health of the Indigenous Peoples in the Americas, recognized the progress made by the Health of the Indigenous Peoples Initiative of the Americas (SAPIA) while acknowledging the persisting inequities in access to health services affecting indigenous peoples.8 In addition, PAHO member states’ approval in 2010 of a specific resolution on health and human rights confirmed a commitment to take into account international and regional human rights norms and standards, including those protecting indigenous children’s rights, as the guiding principles for all health initiatives in the region.9
PAHO member states have also recently approved Resolution CD53.R14: Strategy on Universal Access to Health and Universal Health Coverage, which refers to ethnicity as essential to the core principles and aims of universal care and access, and considers gender, ethnicity, age, and economic and social status as specific social determinants that have a potential positive or negative impact on health inequities.10
Other mechanisms have also been set in place to advance towards ensuring the right of indigenous children to health.11 In 2001, the United Nations Commission on Human Rights appointed a special rapporteur on the situation of human rights and fundamental freedoms of indigenous peoples, subsequently confirmed by the Human Rights Council in 2007. However, although the Council has requested the special rapporteur to pay particular attention to the situation of indigenous children and relevant reports including the situation of indigenous children have been elaborated, these have not to date included or generated specific studies addressing the health of indigenous children.12 Nevertheless, when the United Nations Permanent Forum on Indigenous Issues held its second session in 2003 on indigenous children and youth, states were urged to undertake and promote the expansion of national health systems in order to provide holistic health programs for indigenous children incorporating preventive medical practices and family and community participation.
A rights-based approach to health programs for indigenous children
Although only the CRC’s General Comment No. 11 specifically refers to the right to health of indigenous children, the references to indigenous peoples and to indigenous children within these varied mandates have proven essential tools for promoting country-level actions and for advocacy to accelerate such efforts. The existence of relevant normative frameworks is of crucial significance in mandating countries to act.
Implementing these mandates can, however, be a challenge for many countries, particularly in responding to the specific objectives and principles of rights-based programs aimed at closing health inequities at the heart of these various normative frameworks in the contexts of the complex realities of social, cultural, and economic exclusion faced by indigenous populations in the region; the profundity of the health inequities faced by indigenous children; and the relative weakness of health systems. Rights-based health policies, strategies, and programs are generally understood to be those that aim to progressively eliminate all barriers to the enjoyment of the right to health for all members of a population. Standards and principles to ensure this goal include non-discrimination, availability, accessibility, affordability, and participation.
The precise meanings and applications of these principles with respect to indigenous populations, and particularly indigenous children, can be fraught with complexity but are arguably essential to ensure the success of any particular program targeted towards these communities. In particular, participation cannot be overemphasized, as addressing the health of indigenous children cannot be separated from the social, cultural, and historic contexts in which it takes place. Therefore, any specific health program for indigenous children must offer a community perspective broad enough to address both the needs of children and the local worlds in which they live. Nevertheless, engaging communities in an intercultural dialogue requires a special combination of political will and local capacity that can be difficult to construct, and the engagement of children and their families adds another layer of complexity. Without this engagement, however, even targeted approaches are likely to have limited impact.
Similarly, since cultural barriers can often present the most complicated challenge to overcoming barriers to health for indigenous peoples, intercultural approaches are vitally important. However, there is often little understanding of the social and cultural factors deriving from the knowledge, attitudes, and practices in health of indigenous peoples, thus specific expertise is required to employ participatory methodologies in each context to identify relevant beliefs, practices, and traditions, and ensure that interventions are designed that incorporate these into biomedical approaches to health, to the greatest degree possible.13 Successful examples of such ‘intercultural approaches’ include the incorporation of safe traditional birthing practices in maternal health services in Ecuador and Peru, where the Institute of Social Security offers alternatives in addition to Western medicine, such as traditional medicine. In Colombia, the intercultural approach has been taken a step further in the indigenous hospital of Pueblo Bello, in Valledupar, with 80% of the hospital’s professional staff of indigenous identity/origin.
This incorporation is likely to increase the acceptability—and hence the accessibility—of health services. Indeed, without such intercultural approaches as a fundamental building block of approaches to eliminate health disparities, the cultural rights of specific ethnic groups are arguably not guaranteed and thus health service provisions are discriminatory. The principle of acceptability implies that services must be culturally and socially acceptable. Non-discrimination and equality imply the recognition by the state of different and specific needs of groups facing particular health challenges. The obligation to ensure non-discrimination requires specific health standards to be applied to particular population groups.
Accountability for the right to health: Measuring impact on indigenous populations
Accountability for such rights-based programming, in this respect, clearly includes the need to measure the process of interventions aimed at improving the health of indigenous children as well as equitable outcomes, or at least paying specific attention to the impact of interventions on particularly marginalized target populations (here, indigenous children) in order to ensure that states meet the commitments of the various normative mandates.
Data are therefore crucial to the generation of evidence not only on the generalities of the health of particular groups, such as indigenous children, and to reveal the different scenarios that may leave specific groups of indigenous children unprotected or invisible (such as, for example, migrant indigenous children, or children living in prisons with incarcerated parents) but also to track this process and its results.
However, data disaggregated by ethnicity are notoriously scarce, in part because of the methodological and political complexities of making concrete a concept such as ethnicity in a rigorously comparable variable and thus as a stratifier of health equity. This complexity arises from the nature of the concept itself which, unlike the supposedly biological stratifier of race, has been used to denote groupings of human society “that entertain a subjective belief in their common descent because of similarities of physical type or of customs or of both, or because of memories of colonization or migration.”14 It is then, as Anderson termed it, “an imagined community.”15 Furthermore, the use of the term as a means of identification of a person, or a group, has yet more complex rights dimensions, since this subjective belief, or perception, of belonging to a particular ethnicity can be “claimed by the people themselves [or] attributed to them by others.”16
Great care needs to be taken with, on the one hand, the avoidance of assigning people to an ethnic group (itself a potentially prejudicial act) and, on the other, identifying the ethnic identity of a given person in order to ensure that person does not suffer from discriminatory treatment. Only by including ethnicity as a stratifier in data analysis, and hence in information systems, is it possible to track impact and for the human rights mandates embodied in the various conventions and instruments noted in this article to have true meaning. Without data, it is impossible to hold countries totally accountable for these commitments, and indeed for countries themselves to formulate evidence-informed policies and programs and monitor their effectiveness. Many countries, therefore, are making substantial strides towards the identification of ethnicity as a stratifier and the measurement of ethnic inequities in health, many on the basis of self-identification in attempts to circumvent these issues.
This identification of impact on specific ethnic groups via the inclusion of ethnic identity as a stratifier is of crucial importance to impact measurement and, hence, the success—or otherwise—of health programs in meeting the human rights commitments outlined in the normative agreements. However, above and beyond impact upon ethnic disparities in health, measuring the process (in terms of the ways in which a particular program has incorporated human rights principles of specific relevance to indigenous populations) and any causal relationship between the impacts and the process employed is more complex but equally important.
The Brazilian case
The context of ethnic inequalities in Brazil affecting indigenous child health
The following sections of this article set out some of the means by which Brazil has attempted to institute programs that potentially impact upon indigenous children’s health, highlighting in what way they respond to the principles noted above and what is possible—and not possible—to note in terms of their impact, as well as the complexities of measuring impact, and making linkages between process and impact, in a rigorous way.
Ethnic inequalities in health, and in development in general, are evident in Brazil. The Brazilian Institute of Geography and Statistics (IBGE) data from 2010 show that Brazil has an estimated population of 191 million people, with 63 million under 18 years old. Among these, 29.6 million people live in poverty. The rate of the general Brazilian population living in poverty is 31.5%, and rises to 50.3% when only considering children between 0 and 17 years old. Approximately 11.5 million children are under six years old and live with a monthly income of less than half the minimum wage per capita.
In Brazil, land is an important component of shared notions of cultural identity, as evidenced historically in the land rights struggles of different indigenous groups. In 2016, 611 indigenous lands are recognized; this corresponds to approximately 13% of the national territory. In the Amazon, they account for 25% of the land area and register preservation rates higher than those found in conservation areas. There are approximately 817,000 indigenous in Brazil, distributed in 220 different villages and with 180 different languages. They live in 4,774 traditional communities located in 438 municipalities, a significant challenge to public policies, due to dispersion and their location in regions that are geographically difficult to access. Children living in rural areas are twice as vulnerable to poverty as those living in urban areas.
Brazil’s recognition of indigenous peoples’ rights
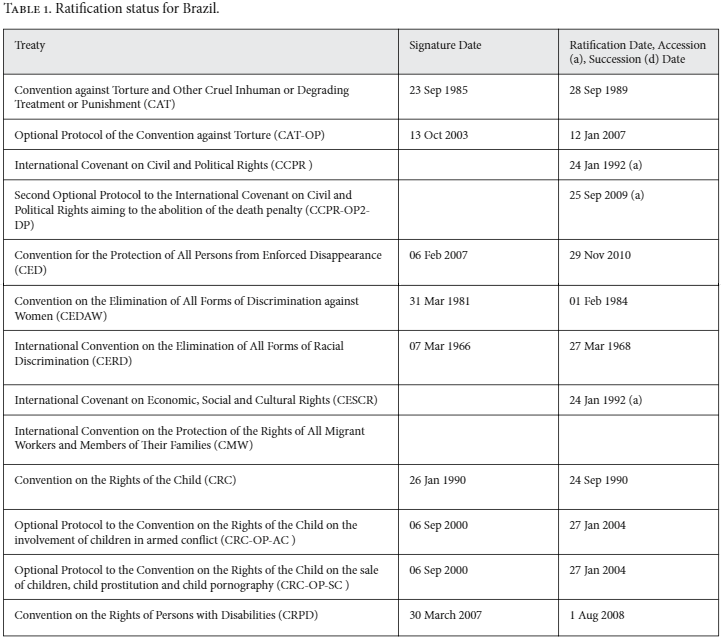
Brazil is a signatory to many relevant international and regional conventions, as shown above. Furthermore, the Brazilian Constitution (1988) explicitly aims to serve as a model in relation to the recognition of rights and fundamental guarantees.17 It recognizes civil, political, economic, social, and cultural rights, and aims to ensure that all these human rights are enforceable in the courts. Under the Constitution, social rights include “health…and the protection of childhood,” and Article 196 defines health as:
a right of all and a duty of the State and shall be guaranteed by means of social and economic policies aimed at reducing the risk of illness and other hazards, and at the universal and equal access to actions and services for its promotion, protection and recovery.
In 1990, the law establishing Brazil’s Unified Health System (SUS) was approved.18 Article 2 of the law also confirmed “health as a fundamental right of the human person” and expressly states that “the State must guarantee the conditions necessary for its full exercise.” This law provides the necessary conditions for promotion, protection, and recovery of health; the organization and operation of the services; and other measures. It regulates actions and health services throughout the national territory.
The Brazilian Constitution recognizes indigenous peoples to have exclusive usufruct rights to the riches of the soil, the rivers and the lakes existing on their lands. Indigenous social organization, customs, languages, creeds, and traditions are also recognized. Achieving development with respect for human rights, in a manner that ensures empowerment of individuals and groups, is explicitly stated as a government priority.
Although challenges remain, including the approval by National Congress of the Statute on Indigenous Peoples, submitted in 2009, these formal rights have translated into progress in promoting the rights of indigenous peoples, particularly between 2008 and 2011. Examples include self-identification of indigenous peoples in the demographic census and the Campaign to Eliminate Unregistered Births, which has a clear impact on the right to health. In 2009–2010, 2,895 collective mobilizations resulted in the issuance of more than 85,000 birth certificates. Most of these efforts occurred in rural areas, and many were aimed at traditional, nomadic, semi-nomadic, gypsies, and homeless communities. In 2016 only 6% of Brazilian children aged between one and two years lack birth certificates.
Operationalizing the human rights agenda on indigenous child health in Brazil
It is widely recognized that the best development policy for Brazil is to combat poverty, while the best human rights policy is to reduce inequality and discrimination among people, regions, races, and genders.xix Brazil’s approach has been designed to confront both these development and human rights challenges. Since 2003, Brazil has made poverty eradication a key priority and, with a view to reducing both poverty and social inequality, has integrated social policies into economic growth strategies, fostering sustainable and inclusive development.
In 2003, the Brazilian Government adopted the Fome Zero network of federal assistance programs with the goal to eradicate hunger and extreme poverty in Brazil. Within the Fome Zero strategy, the Programa Bolsa Família, established by Law 10,836 in 2004, attempts to both reduce short-term poverty by direct cash transfers and fight long-term poverty by increasing capacities through conditional cash transfers. Among the conditions of the program, families must ensure that children attend school and are vaccinated. The government has recognized that this program has contributed significantly to the reduction of poverty in the country, from 7.6 % in 2004 to 3.6% in 2012 (PNAD 2012) and has also contributed to declines in income inequality.20 Between 2001 and 2009, the ratio of household per capita income of the richest 20% against the poorest 20% dropped from 24.3 to 17.8.21
It is clear, then, that Brazil’s approach has been to understand equality as a key dimension of human rights. As such, instruments have been developed to confront a reality in which differences based on gender, race, age, religion, sexual orientation, and other factors, affect access to public policies, and the realization of rights, including those related to health. Actions to reduce vulnerability have been incorporated into state initiatives in areas provided for under the Third National Human Rights Programme (PNDH-3), including poverty reduction, promoting adequate food, health, education, agrarian reform, combating violence in the countryside, eradicating child and slave labor, promoting women’s rights, and, of key relevance here, promoting the rights of indigenous and quilombo communities to full and effective participation.
Institutional structures relevant to indigenous child health in Brazil
In order to implement these strategies, programs, and instruments, Brazil has established a series of institutional structures relevant to the promotion of indigenous child health. The Subsystem of Attention to Indigenous Health was established by the 1999 Law No. 9836/99 (Arouca Law), under the Unified Health System (SUS) to ensure indigenous peoples the right to universal access. Importantly, in terms of process, these assurances are accompanied by respect for ethnic and cultural diversity. The system is organized through 34 Special Indigenous Health Districts (DSEI), with the responsibility to structure and coordinate the health care network within territories in an integrated and hierarchical manner, and importantly for intercultural approaches, incorporating indigenous traditional practices. As well as the technical areas of Child Health and Breastfeeding and of Adolescent and Youth Health, a Special Secretariat for Indigenous Health was established in 2010.
Interventions targeting indigenous child health in Brazil
The Government of Brazil, and particularly the Health Sector, clearly considers this constituency as a priority area. Integrated as well as targeted interventions have been designed and implemented. The Care Policy on Indigenous Health prioritizes health promotion activities, prevention, and control of diseases and disorders, based on the epidemiological profile of the indigenous population, characterized by a high incidence of respiratory and acute gastrointestinal infections, malaria, TB, sexually transmitted diseases, malnutrition, skin diseases, and vaccine-preventable diseases.
The attention given to combating the principal health issues identified via epidemiological profiling of indigenous groups is laudable and in itself an effort to redress inequities and thus guarantee the right to health for all. However, even this prioritization process and the targeted approach is not without its potential pitfalls from a rights perspective. For example, it is unclear to what degree indigenous populations themselves were involved in this process of agenda setting. Similarly, such targeted efforts necessarily require the identification of indigenous communities with respect to their epidemiological profile which, while necessary to identify health intervention priorities also may be questioned as to the political dimensions of such explicit targeting, as opposed to efforts to target communities on the basis of poverty and other aspects of socio-economic exclusion.
Other initiatives have been less explicitly ethnically specific and have focused instead on impoverished populations. Of significance, for instance, in attempts to tackle the issue of indigenous child health in Brazil is the Family Health Program, which is one of the world’s biggest programs for promoting door-to-door family health care. It involves initiatives of the federal government, 27 states, and 5,264 municipal governments, with more than 220,000 community health workers giving attention to 110 million people, especially in impoverished areas. Since 2011, the government has significantly increased its investments in the program, which represents the greatest guarantee of supply of basic care in the history of public health in Brazil. Despite not being specifically targeted to indigenous populations, they are likely to have significantly benefited due to their overrepresentation among those living in contexts of poverty.
The model of health care prioritizes actions on the principles of territoriality, mainstreaming, decentralization, and shared responsibility, and population groups with a higher risk of disease or death. Hence, especially with respect to decentralization and shared responsibility, the principles of participation, acceptability, and accessibility should have also been key components. It is difficult, however, to determine to what degree the means of implementation may or may not have affected results, given the lack of specific focus on indigenous communities.
This strategy was strengthened in 2014 by the establishment of Mais Medicos para o Brasil, a program that hired more than 15,000 foreign and Brazilian doctors who have studied outside of Brazil. Initial preliminary results appear to show increases in the population coverage of the Family Health Program, suggesting that this intervention will impact maternal and child mortality. This initiative has opened up possibilities to track at least health care coverage (and to some extent, access and outcomes) for indigenous communities. For example, 305 doctors were assigned to indigenous communities, and significant impacts on health indicators among these populations are therefore expected.
Although not explicitly focused upon indigenous populations, the Family Health and the Mais Medicos programs align well with existing initiatives under the Special Secretariat for Indigenous Health, which by December 2014 had established the indigenous health network, including 4,108 indigenous health agents and 2,010 indigenous sanitation agents, besides doctors, nurses, and other health care professionals. As of April 2016, there are around 12,813 professionals working in the 34 sanitary indigenous districts, 200 doctors, 1,414 nurses, and 3,225 nursing assistants. The targeted approach to indigenous districts as well as the deployment of individuals specifically aimed at overcoming the barriers to health in these particular contexts should increase the probability not only of impact (in terms of coverage, access, and outcomes), but also of a process that takes into account the specific human rights concerns within such communities. However, limited evidence is available in that respect.
Integrated Management of Childhood Illness (IMCI)
It is obvious, then, that the potential disadvantage of programs not specifically focused on indigenous communities is the limitation on the focus on rights within the process (or at least the difficulties with ascertaining this within a non-targeted approach). Other strategies to promote indigenous children’s health involved a combined approach, incorporating components of participation in more generalized strategies, and perhaps represent a comfortable medium point between the two polarities of approach.
Brazil’s IMCI strategy to address indigenous child health adopts an integrated approach to the management of childhood illness, which is also based upon participation and interculturality. It aims to reduce death, illness, and disability, to promote improved growth and development among children under five years of age, and includes both preventive and curative elements that are implemented by families and communities as well as by health facilities.
For this purpose, intercultural approaches to health have been put in place. In particular, with the support of PAHO, the country has established a group of indigenous health specialists focused on the IMCI Strategy. Around 130 specialists are distributed among all indigenous sanitary districts to conduct capacity building. Although the material used is the same as that used for non-indigenous children, the approach in these areas is also an intercultural one, with open dialogue promoted between the different cultures, and indigenous peoples participating in decisions impacting the community. This strategy has been viewed by the government as a priority for the reduction of child mortality among the indigenous population, and the many factors that may particularly put indigenous children at specific serious risk are evaluated in a participatory way. It is important to note here that the principle of effective participation entitles indigenous people to a right not only to be consulted, but to be involved to the point of giving or withdrawing consent. Hence, the very fact that indigenous peoples accept their children to be involved in such programs and to receive immunization (see below) reveals the impact that a continuous dialogue can have on the health outcomes of particularly hard to reach, ethnically marginalized communities.
Immunization: A targeted approach to improving the health of indigenous children in Brazil
Such approaches reveal an understanding of the need to adopt an intercultural participatory approach to health, when focusing upon indigenous children within more generalized programs and that, through such processes, programs optimize their potential for impact, as well as complying with the principles of human rights programming. Some of the most palpable impacts upon indigenous children’s health, however, have been achieved by instituting a targeted approach, which has allowed not only for explicit targeting of this particular population group but also the possibility of putting into place a process that respects the intercultural approach to health and takes into account the realities of their lives and living conditions.
The latter has been perhaps most notably achieved in the National Programme for Malaria Control, established in 2003, which seeks to improve immunization of indigenous children as well as access to diagnosis and early treatment. The operation of the immunization system established for indigenous peoples, including children, is complex due to several factors, such as geographical dispersion of indigenous communities, high turnover of human resources, difficulties in packaging and suitable transport biopharmaceuticals, and deficiency of information generated in the various levels of management.
In order to help address these issues, the Ministry of Health, through 2013 Ordinance No. 1798, defined the national indigenous immunization calendar. This calendar provides the structure for application of a number of vaccines at different ages among the general population, with the aim of promoting greater protection for indigenous children, taking into account the vulnerable conditions in which they live. During this month, all health teams make an additional effort to support communities in the most remote areas and where the immunization coverage is lowest. As much as the practical aspects involved in its application, however, the specific month for vaccination of indigenous peoples in Brazil allows for particular attention to be given to specific health standards to be applied to particular population groups, in full accordance with human rights principles. It also recognizes the state’s duty to meet the different and specific needs of groups facing particular health challenges, as implied by the principles of non-discrimination and equality. This includes the principle of acceptability with respect to services being configured in culturally and socially acceptable ways.
The following risk criteria are used to identify priority areas:
1) Areas of difficult geographic access;
2) Low vaccination coverage;
3) Quality problems in the immunization information system;
4) Occurrence of vaccine-preventable diseases;
5) Less than three vaccination stages in the last year.
During the Vaccination of Indigenous Peoples month, a national campaign of vaccination against influenza is also held, seeking to vaccinate the entire indigenous population aged from six months. The month is also an opportunity to upgrade indigenous peoples’ vaccination cards, especially in areas of difficult geographic access.
This strategy has contributed to a 30-40% annual increase in vaccination coverage, which is highly significant given that epidemiological studies worldwide show that vaccines are efficient measures of disease prevention and reduction of mortality, especially among children. Studies have also indicated that high immunization coverage is an indicator of the quality of health services and serves as a relatively simple means of verifying access to health services. These efforts by Brazilian authorities, as well as of individual health professionals working with the communities, may therefore be seen to demonstrate the commitment to offer quality services and to guarantee the right for health to all, especially indigenous children.
Impacts of Brazil’s integral and targeted attention to indigenous children’s health
As previously noted, it is a challenge to measure the impact of these varied initiatives. However, one distinct advantage of Brazil’s attention to the issue of indigenous rights is their recognition that ensuring accountability for meeting the commitments to indigenous rights, as enshrined in the various relevant normative conventions and protocols, means identifying ethnic variables in information systems.
Despite the political complexities, such identification allows for tracking and monitoring ethnic inequalities in health and the success, or otherwise, of programs, in terms of their impacts on closing the health gap between indigenous and non-indigenous populations. The National Indian Foundation (FUNAI) of the Ministry of Justice is responsible for systematizing information regarding the Brazilian indigenous population and, in 2007, registered a population of at least 175,365 indigenous children up to 14 years old, of whom 3,627 were aged less than one year.22
The explicit identification of this population as a visible group for priority attention makes it is possible, at least partially, to track impacts upon indigenous children’s health. Brazil has been moving towards this inclusion of ethnic variables and hence over recent years has been attempting to identify some results of its interventions. However, data disaggregated by ethnicity are often still not available and geographical area is frequently used as a proxy for tracking results on indigenous populations. The limited nature of the impacts also shows that, despite advances, the precise formula for impacting upon indicators related to indigenous children’s health has not yet been found.
Infant mortality rates
According to the state’s report presented to the Committee on the Rights of the Child, from 1990 to 2007, the infant mortality rate has shown a tendency for decline throughout the country (47.1 to 19.3/1000), with an average reduction of 59% (a reduction of -4.8% per year). However, in the 2006 analysis of the causes of death in children aged less than one year, it was observed that 71% of the deaths were avoidable, and this percentage has remained unchanged since 1997. Data that use ethnic identity as a stratifier have shown that, although the trend is decreasing, indigenous infant mortality rate is not decreasing at the same expected speed.
Nutrition
Malnutrition in children aged less than one year dropped by more than 60% from 2002 to 2007. The number of malnourished children under two is also decreasing. The proportion of children with low weight for their age dropped from 13% to 3% between 2000 and 2006, representing a 72% reduction. However, the prevalence of children under two with low weight is four times higher in the northeast region than in the south region, reflecting conditions associated with poverty and inequality, particularly within indigenous populations.
Malaria and other infectious diseases
There was a reduction of deaths from infectious diseases, parasitic diseases, and acute respiratory infections in children under five from 14.8% to 12.3% in 2007. The total number of cases of malaria in children and adolescents was 408,821 in 2003, reaching its peak in 2006, with 605,026, and falling back to 456,809 cases in 2007. Despite these achievements, and the inference of results of programs primarily focused on indigenous populations, no specific information is available on indigenous children affected by malaria.
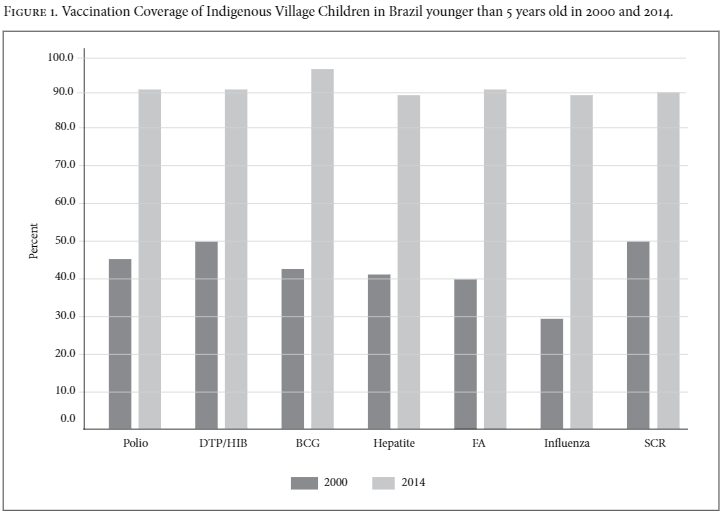
Immunization
Immunization has had the most success in terms of clear impact upon indicators. A gradual increase in vaccination coverage is observed in the greater regularity of routine vaccination activities, including those focused on indigenous populations. Figure 1 shows the increase in vaccination coverage of the main vaccines used in children aged under five between 2000 and 2014.
Conclusion
Both the integrated and intersectorial interventions, as well as targeted approaches, applied by the Brazilian government are impacting the health indicators of indigenous children and respond to the various UN conventions and other normative frameworks and mechanisms identifying the health of indigenous children as a human rights concern, particularly the CRC and its specification of indigenous children’s rights. Vaccination coverage specifically addressing indigenous peoples is a clear example of commitment to the human rights obligations of the country, and is one particular area where impacts on indigenous children’s health are clear.
What is unfortunately not so clear, and currently not feasible to measure, is to what degree the process of implementation affects these impacts. However, although not necessarily consistent nor universal, human rights health programming principles, including availability, accessibility, and acceptability, have been components of the implementation process during many of these interventions. Of particular significance to the intercultural approach, many programs have been formulated with the direct participation of indigenous peoples. Hence, they respond to mandates relating not just to the need for improved health outcomes and access to health as a right but also for the process to be rights based. Nevertheless, these impacts across all health indicators are, to date, neither as consistent nor as significant as in other populations, showing that the precise formula has yet to be identified to best impact upon the health of marginalized ethnic populations, such as indigenous children. An even greater degree of attention to the incorporation of intercultural approaches in the future is likely essential in order to fully take into account the unique individuality of each group and provide a specific, appropriate, and adequate response to the needs of indigenous children’s health in each context.
Nevertheless, despite these reservations, and although the operationalization of human rights varies from one country to another, Brazil’s experiences illustrate how interventions using human rights approaches can potentially improve the health of indigenous children and may constitute interesting examples for other countries in the Americas and beyond, to replicate and adapt to their own contexts. Brazil has also made important strides in data collection to facilitate identification of health inequities between ethnic groups and to track the impact of programs aiming to confront these inequities, and thus be held accountable for addressing them.
Challenges still exist. Although the sum of all the interventions appears to be having an effect and we can assume that at least some elements of the human rights approach play a significant role, the lack of rigorous evaluations using ethnicity as a stratifier for individual programs makes it difficult to assess what influence the individual program design has had. Brazil’s advances in including ethnicity data in health and other information systems are certainly positive and constitute the country as a regional leader but there is still limited ability to identify concrete results for specific ethnic populations, thus highlighting the need for Brazil, and other countries, to further grapple with the methodological and political challenges and more systematically collect data and evaluate impacts using ethnicity as an analytical category.
The inclusion of a target on data disaggregation within Goal 17 of the Sustainable Development Goals (SDGs), and specifically within the area of data, monitoring, and accountability, is a positive step towards this aim. The target calls for “enhance[d] capacity building support to developing countries, including for LDCs and SIDS, to increase significantly the availability of high-quality, timely and reliable data disaggregated by income, gender, age, race, ethnicity, migratory status, disability, geographic location and other characteristics relevant in national contexts.”23This target will hopefully provide further impetus to countries in their efforts to identity health inequities affecting indigenous children, and evaluate their efforts at closing these gaps in line with the SDG agenda of inclusion and universality, within the framework of “no one should be left behind” and “no target should be met, unless met for all groups.”
Alongside this new agenda, it will also be important to reinforce the existing human rights mechanisms that make it possible to assess the vulnerability of particular situations and groups, and on their basis, advocate for further specific laws, policies, and programs to be adopted with the goal of improving the health of indigenous children, as well as guaranteeing their other related human rights. The limited available evidence shows that there is an urgency for increased evidence and for accelerated action, and thus for international mechanisms to not only generate relevant studies that take into account the different realities, opinions, and best interests of indigenous children but also to adopt a far more specific focus on the health of indigenous children. To date, only the Committee on the Rights of the Child, through its General Comment No. 11, analyzes the right to health for indigenous children. More evidence and analysis is required to formulate effective state responses that guarantee the human rights of indigenous children. This necessitates much more effective and rigorous measurement methodologies in ethnicity and health so the impacts of human rights based health programming can be assessed, and to ensure accountability for commitments to close this widest of health inequities affecting indigenous children.
Anna R. Coates is the Chief of the Gender and Cultural Diversity Unit at the Pan American Health Organization/World Health Organization, Washington DC, USA.
Sandra del Pino Marchito is the Cultural Diversity Advisor at the Pan American Health Organization/World Health Organization, Washington DC, USA.
Bernardino Vitoy is the Specialist on Family and Community Health at the Brazil Office of the Pan American Health Organization/World Health Organization, Brasilia, Brazil.
Please address correspondence to Anna R. Coates, Email: coatesa@paho.org
All authors are staff members of the Pan American Health Organization. The authors alone are responsible for the views expressed in this publication, and they do not necessarily represent the decisions or policies of the Pan American Health Organization.
© 2016 Pan American Health Organization; licensee Health and Human Rights Journal. This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial IGO License (http://creativecommons.org/licenses/by/3.0/igo/legalcode), which permits distribution and reproduction in any medium, for non-commercial uses provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that PAHO or this article endorse any specific organization or products. This notice should be preserved along with the article’s original URL.
References
- Department of Economic and Social Affairs (DESA), State of the World’s Indigenous Peoples. United Nations: New York, (2009). Available at: http://www.un.org/esa/socdev/unpfii/documents/SOWIP/en/SOWIP_web.pdf
- UN Committee on Economic, Social and Cultural Rights, Concluding Observations to Brazil, UN Doc. E/C.12/BRA/CO/2 (2009). Available at: http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=E/C.12/BRA/CO/2&Lang=En
- UN Committee on the Rights of the Child, General Comment No. 11, Indigenous Children and their Rights under the Convention, UN Doc. CRC/C/GC/11 (2000). Available at: http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=CRC%2fC%2fGC%2f11&Lang=en
- UN Committee on the Elimination of Racial Discrimination, Concluding Observations to Brazil, UN Doc. CERD/C/64/CO/2 (2004). Available at: http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=CERD/C/64/CO/2&Lang=En
- ILO Convention No. 169, International Labour Organization (1989). Available at: http://www.ilo.org/indigenous/Resources/Publications/WCMS_100897/lang–en/index.htm
- UN Committee on the Rights of the Child, Day of General Discussion on the Rights of Indigenous Children (2003). Available at: http://www.ohchr.org/Documents/HRBodies/CRC/Discussions/Recommendations/Recommendations2003.pdf and UN Committee on the Rights of the Child, General Comment No. 11, Indigenous children and their rights under the Convention (2009). Available at: http://www2.ohchr.org/english/bodies/crc/docs/CRC.GC.C.11.pdf
- Pan American Health Organization/World Health Organization, Health of Indigenous Peoples, Doc No. CD40.R6, Health of the Indigenous Peoples of the Americas (1997). Available at: http://www.paho.org/hq/index.php?option=com_docman&Itemid=1358&lang=es
- Pan American Health Organization/World Health Organization (PAHO/WHO), Health of the Indigenous Peoples in the Americas, Doc No. CD47.R18. Available at: http://www.paho.org/hq/index.php?option=com_docman&Itemid=1358&lang=es
- Pan American Health Organization/World Health Organization (PAHO/WHO), CD50/12 and CD50.R8 of the 50 PAHO Directing Council (2010), Health and Human Rights, available at http://www2.paho.org/hq/dmdocuments/2010/CD50-12-e.pdf
- Pan American Health Organization/World Health Organization (PAHO/WHO), Strategy for Universal Access to Health and Universal Health Coverage, Doc No. CD53/5, Rev.2 of the 53 PAHO Directing Council (2014). Available at http://www.paho.org/hq/index.php?option=com_content&view=article&id=9774&Itemid=41062&lang=en
- UN Committee on the Rights of the Child, Concluding Observations to Brazil, Doc No. CRC/C/15/Add.241 (2004). Available at: http://tbinternet.ohchr.org/_layouts/treatybodyexternal/Download.aspx?symbolno=CRC%2fC%2f15%2fAdd.241&Lang=en
- Special Rapporteur on the Rights of Indigenous Peoples, information on thematic and country reports. Available at: http://www.ohchr.org/EN/Issues/IPeoples/SRIndigenousPeoples/Pages/SRIPeoplesIndex.aspx
- Pan American Health Organization/World Health Organization (PAHO/WHO), CD47/13 of the 47 PAHO Directing Council (2006), Health of the Indigenous Peoples of the Americas. Available at: http://www1.paho.org/english/gov/cd/CD47-13-e.pdf
- M. Weber, (1968) Economy and Society, University of California Press
- B. Anderson, (1983) Imagined Communities: Reflections on the Origin and Spread of Nationalism. (London: Verso)
- Guibernau and Rex (1997), The Ethnicity Reader: Nationalism, Multiculturalism and Migration, Cambridge: Polity Press, 1997
- Brazilian Constitution (1988). Available at: http://pdba.georgetown.edu/Constitutions/Brazil/english96.html
- Law 1990, establishing Brazil’s public health system, the United Health System (SUS), Lei Nº 8.080, 19 September 1990. Available at http://www.planalto.gov.br/ccivil_03/leis/l8080.htm
- National Report submitted in accordance with paragraph 5 of the annex to Human Rights Council resolution 16/21, Brazil, UN Doc No. A/HRC/WG6/13/BRA/1 (2012). Available at: http://www.ohchr.org/EN/HRBodies/UPR/Pages/BRSession13.aspx
- UN Committee on the Rights of the Child, Consideration of reports submitted by States parties under article 44 of the Convention, Doc No. CRC/C/B/RA/2-4, 2014. Available at: http://tbinternet.ohchr.org/_layouts/TreatyBodyExternal/Countries.aspx?CountryCode=BRA&Lang=EN and National Household Sample Survey (PNAD), 2012
- IBGE. Síntese de indicadores sociais: Uma análise das condições de vida da população brasileira 2010 (Summary of Social Indicators: A review of the living conditions of the Brazilian population 2010). (Rio de Janeiro: IBGE, 2010).
- National Indian Foundation. Available at: http://www.survivalinternational.org/about/funai
- Transforming Our World: The 2030 Agenda for Sustainable Development – Finalised Text for Adoption (1 August), available at: https://sustainabledevelopment.un.org/content/documents/7891Transforming%20Our%20World.pdf