Data-Driven Human Rights: Using the Electronic Health Record to Promote Human Rights in Jail
Sarah Glowa-Kollisch, Kelly Andrade, Richard Stazesky, Paul Teixeira, Fatos Kaba, Ross Macdonald, Zachary Rosner, Daniel Selling, Amanda Parsons, Homer Venters
Health and Human Rights 2014, 16/1
Abstract
The electronic health record (EHR) is a commonplace innovation designed to promote efficiency, quality, and continuity of health services. In the New York City jail system, we implemented an EHR across 12 jails between 2008 and 2011. During the same time, our work increasingly focused on the importance of human rights as an essential element to the provision of medical and mental health care for our patients. Consequently, we made major modifications to the EHR to allow for better surveillance of vulnerable populations and enable reporting and analysis of patterns of abuse, neglect, and other patient concerns related to human rights. These modifications have improved our ability to find and care for patients injured in jail and those with mental health exacerbations. More work is needed, however, to optimize the potential of the EHR as a tool to promote human rights among patients in jail.
Introduction
In the US, approximately 10 million people cycle through jails and prisons annually, with 90% of these incarcerations occurring in jails. Incarcerated persons tend to be poor, from racial and ethnic minorities, and have high rates of medical, mental health, and substance abuse problems.1,2 In addition to having high rates of pre-existing health concerns, the incarcerated face new health risks during incarceration, including injury from violence and mental health stressors.
Like community health settings, correctional health systems are beginning to adopt electronic health records (EHR) as tools for promoting safe, reliable care. Commonly cited advantages of EHRs include better coordination of care between providers, reduction of unnecessary tests and procedures, reduction of paperwork, and direct access to patient health records when out of the office.3,4 In correctional settings that have adopted an EHR, clinical staff and their patients benefit from accessibility to records from prior incarcerations. In addition, integrating mental health and medical care is key for correctional EHRs.
In the New York City (NYC) jail system, security is the responsibility of the NYC Department of Corrections (DOC), while health care is the responsibility of the Bureau of Correctional Health Services (CHS) of the NYC Department of Health and Mental Hygiene (DOHMH). The NYC jail system is the nation’s second largest, with 12 jails housing approximately 12,000 inmates on any given day, and representing 80,000 annual admissions. Although the average length of stay in the NYC jail system is approximately 45 days, the median stay is just eight days. Consequently, the jails are chaotic settings where large quantities of information are gathered and care is delivered, and where taking a comprehensive and holistic approach to care is difficult. Without an EHR, it is extremely difficult to pull together sufficient details to detect vulnerability among patients who are subject to abuse or neglect, or to identify those with special needs and to act in a manner to quickly protect them.
We began the adoption of an integrated EHR in the NYC jail system in 2008, and completed this process in 2011.5 An ambulatory (outpatient) EHR, eClinicalWorks, was selected for this process, which required substantial modification of the core product to meet the needs of our system. In particular, the EHR was substantially modified for new admission intakes, sick call, medical emergencies, infirmary care, medication dispensation, hemodialysis, newborn nursery, mental health encounters, and solitary confinement rounds. After a three-year rollout, the EHR has been well accepted by patients and staff as an important tool for improving clinical care. The EHR is used for all aspects of medical, mental health, and discharge planning services, amounting to approximately 30,000 documented patient encounters every month.
The adoption of the EHR highlights concerns for vulnerable populations in the jail system. In response to several adverse outcomes, CHS adopted a health care mission in 2012 that is based on three aims: patient safety, population health, and human rights.6 While the EHR is a key component of each aim, in this paper we suggest that its contribution to the promotion of human rights in the correctional health setting is its most novel and unanticipated strength.
Human rights in correctional health services
Various EHR functionalities support each of the three recently adopted priorities. The first priority, patient safety and health, refers to the need for medical policies and procedures that are consistent with community standards of care and quality assurance and improvement (QA, QI). The EHR is routinely used to gather data collected during the QA/QI process. The second aim, population health, focuses on the need for robust surveillance of disease states and risk factors, as well as trends in morbidity and mortality across the entire jail health system. The EHR is often customized to collect data in a structured way such that it can be analyzed and reported. The third aim, human rights, is a newly adopted objective of CHS and requires significant assessment, training, and intervention throughout all aspects of the CHS operation. Because of the newness and unfamiliarity of these concepts for our staff, we have decided to make human rights a discrete focus, despite its importance to all aspects of our health system. Some human rights concepts incorporated into CHS operations are dual loyalty (the erosion of the medical mission as a consequence of the security setting) and stewardship (maintaining and using an independent health authority). More traditional components of medical ethics, such as beneficence, non-maleficence, autonomy, and confidentiality are also important to the overall human rights framework.
Thus far, the human rights component of the CHS mission has demonstrated three distinct features. First, a high-level forum was created called the human rights collective. This meeting convenes every three months and includes a wide range of experts from clinical, academic, human rights, policy, and advocacy settings to advise on broad topics. We have held five human rights collectives on topics including incarceration and human trafficking, solitary confinement, traumatic brain injury, and structural violence in the jails.
The second element of the human rights operation involves transferring recommendations of the human rights collective into a specific project for a new Human Rights Subcommittee. This subcommittee is part of the overall QI structure of CHS and comprises clinical and operational leaders from the jails, including leadership in nursing, medicine, mental health, operations, and discharge planning. Once the Human Rights Subcommittee identifies and implements a project, the results are reported back to the overall QI committee of CHS.
The final step involves changes to policies, training, or other features of clinical care. The subcommittee recently designed and implemented mandatory online dual loyalty training for all health staff. This training introduces all current health staff to basic concepts of human rights and then presents several dual loyalty scenarios related to correctional health. All newly hired health staff also participate in this training. In addition, the subcommittee maintains a dedicated CHS Human Rights email account where staff may report any concerns regarding these matters. Fully integrating current and/or formerly incarcerated persons in all levels of this process remains an important next step.
Adapting the EHR to vulnerable populations
In correctional settings, the potential harms that can befall patients are not equally distributed. Most correctional settings have mechanisms for protecting vulnerable inmates, such as protective custody. However, patients who are repeatedly victimized often report that they are still vulnerable in these and other settings designed to protect them. Often, health providers have knowledge of individual cases relating to abuse or violence, but without training and technical capacity to link these individual cases to aggregate data analysis, trends may not be detected. In addition, front line providers face a complex set of pressures and may be disincentivized from reporting abuse. Traditionally vulnerable populations in correctional settings include lesbian, gay, bisexual, and transgender (LGBT) patients; patients with mental illness; those reporting injuries; and those in solitary confinement. In the NYC jail system, we have tailored our EHR to allow for surveillance of some of these patient cohorts. The basic steps involved in these modifications include determining what “visit type” the patients may have that relates to their vulnerability, then building templates with structured questions for providers to address. The final step is the production of reports that allow CHS to monitor change in the incidence of health outcomes associated with victimization as well as ensuring the correct use of these visits/templates. This reporting can simply involve counting visit types or can include queries about data elements within specific templates in those visit types.
The first vulnerable population that CHS addressed in this manner was patients injured in jail. In 2008, an adolescent in jail was determined to have been beaten to death. In the investigation and reporting process, it became clear that the facility where the homicide occurred had seen a rise in hand and jaw fractures in the months prior. This information led CHS to undertake an exhaustive review of paper injury reports in 2009-2010. Injury rates were calculated by facility, in a manner consistent with injury reporting done in the community by the Centers for Disease Control and Prevention (CDC).7 This review found the injury rate in the NYC jail system to be higher than the community injury rate. Also, the review identified ‘slip and fall’ as a leading cause of injury, creating a concern that many injuries go misreported out of fear for reprisal.
This injury analysis served as the basis for creating our injury surveillance system in the EHR. Developing a specific injury template for use when caring for injured patients served as a central element of building an EHR-based injury surveillance. The structured variables in the injury template included patient-reported data around intentionality, person causing injury (e.g., correctional staff, inmate, self), and location where the injury occurred (e.g., bathroom, hallway, clinic). Each provider evaluating a patient for injury merges the template into their encounter, which is also specifically categorized as an injury visit. Since the adoption of the EHR, CHS has been able to track the number of injury visits and the share of those visits in which the injury template was correctly utilized and merged. Initial use of the template during injury visits was 50-60% across facilities, but regular monitoring, including reports of providers who had multiple injury encounters but did not properly use the injury template, raised this compliance to approximately 75% in the first 18 months. Subsequent to the rollout of the EHR and injury template, we added two variables to the template. In 2012, we added a question for ‘verified injury.’ The overall number and trends of injury visits is important because they consume significant clinical resources and often displace other clinical activities. However, the ‘verified injury’ rate shows the true clinical burden of injury. Correctional staff may bring patients for injury visits that do not have an actual injury, such as after a use of force or after a large fight. Approximately 45% of all injury visits involve a verified injury. In addition to identification of verified injuries, the EHR allows for the flagging and reporting of serious injuries (verified injuries that include fracture of any bone, need for sutures, or transfer to a higher level of care).
The second change to the injury template involved adding three questions related to traumatic brain injury. These questions include whether the patient was hit in the head, whether the patient lost consciousness, and whether the patient was dazed and confused. These three inquiries approximate mild traumatic brain injury (MTBI, or concussion) and are being implemented to track patients needing further intervention and create an incidence rate of MTBI within the jail system.8 The initial question of whether the patient was struck in the head is also a critical variable in reporting to correctional leadership on the frequency and nature of use of force injuries.
For patients with serious injuries, CHS leadership uses the EHR to review cases on a daily basis to ensure that patients’ injuries were appropriately treated and documented and that follow-up care is in place. It includes a review of previous injuries and mental health visits to identify patients who may need broader interventions, such as consideration for protective custody or compassionate release. When patients report injuries stemming from misconduct by correctional staff, these cases are referred to partner agencies, who are charged with investigating wrongdoing in the jail system. In addition to monitoring proper care of patients, this daily review ensures that both partner agencies (DOC and DOHMH) have sufficient information to properly classify the severity of injuries. CHS leadership spends approximately one hour per day conducting this review of each day’s injuries. Approximately 2,000 injury visits occur each month, with 600-800 involving a verified injury and about 150 being classified as serious injuries.
In the aggregate, the EHR allows for reporting of injury type and location across time and facility. Reports are submitted regularly to the DOC for consideration of security measures and concerns. Reports are also produced that reflect rates of injury by person causing the injury (e.g., inmate, staff, self). These reports allow for both CHS and DOC staff to target interventions toward staff or patients who may be associated with higher rates of overall injury or higher rates of specific types of injury. Examples include self-harm associated with solitary confinement and head trauma associated with use of force. Another use of these reports is allocation of staffing. When injury rates are high in a facility, the staff may have less opportunity to conduct medical follow-up, nursing, and other types of care due to the immediate demand of caring for the injured as well as the need for DOC to conduct security operations that may restrict patient movement and clinic access.
A critical subset of injury reporting and surveillance involves patients reporting sexual assault. Any staff in the health system who are made aware of any allegation of sexual abuse are required to immediately inform central operations staff. This mandate reflects the provisions of the Prison Rape Elimination Act as well as CHS policy. Operational staff then make all mandatory notifications, document these on a checklist, and trigger the visit type in the EHR. The use of the operational checklist and the injury template in the EHR allow supervisory staff to detect when patient evaluation may be incomplete. For example, medical and mental health staff must evaluate all patients who report sexual assault. Real-time reporting of incidents through the operations notification process allows leadership of both medical and mental health providers to verify encounters. The EHR has also allowed for targeted contacts with patients in groups more likely to report sexual assault, including LGBT patients.
Patients with mental illness are a second vulnerable population for whom modification of the EHR allows for increased surveillance. In the NYC jail system, approximately 35% of all men and 60% of all women receive mental health services. As in the community, there is a broad range of mental illness, ranging from mild illness requiring some clinical contact and possible medication, to serious mental illness, requiring housing in a dedicated mental health unit and daily clinical and group encounters, or even hospitalization. Given the size of the mental health service, a real concern of clinical staff is losing track of patients who are faring poorly and require changes in treatment plan or housing area, or who require case conferencing with medical or discharge planning staff. Prior to the implementation of the EHR, separate paper charts were maintained for medical and mental health care. With the rollout of the EHR, which was an ambulatory medical product adapted for jail setting, significant work was required to build templates for mental health encounters. The basic visit types include the initial mental health intake assessment, a treatment plan review, and medication review.
Tailoring the EHR to mental health care was particularly challenging. Because mental health providers record significant amounts of narrative and free text assessment, their encounters are not easily distilled to a series of structured data elements that can then generate reporting. Accordingly, CHS broadened the number of mental health visit types to provide greater specificity. For example, visit types for suicide watch and self-harm gesture were added. In addition, a visit type was created for decompensating patients. In the example of self-harm, individual patients are seen by a mental health and medical provider as soon as their act of self-harm is noticed or reported. The visit type and template utilized by the mental health staff in these encounters allows for aggregated reporting on locations of self-harm, type of self-harm, lethality, pre-existing diagnoses, and medications. This capacity for aggregate reporting recently allowed us to complete an analysis of self-harm across approximately 245,000 jail admissions. This revealed that adolescence, serious mental illness, and solitary confinement are all highly associated with self-harm in jail, with odds ratios of 7.5, 8.0, and 6.9, respectively.9
CHS also has dedicated templates and visit types for patients tracked for drug and alcohol withdrawal, as well as for patients receiving methadone detoxification or maintenance therapy. Finally, discharge planning staff in the mental health service also use the EHR with structured templates that allow for reporting of discharge plan initiation and completion of associated tasks.
The capacity of the EHR to track patients in solitary confinement is an important area of development for patients with mental health concerns. Currently, medical and mental health staff conduct thousands of rounds each day, checking on patients who are locked in cells for most of the day. These rounds are an imperfect adaptation to the security setting. Staff are asked to pass by a cell, speak briefly with a patient through a large door, and assess whether they are decompensating from a medical or mental health standpoint. If a patient has covered the door with a towel or if he or she refuses to engage verbally, staff can ask for the patient to be removed from the cell for a more significant encounter. However, this action requires time and resources from security staff. Security and health staff face significant disincentives to opening cell doors or removing patients to a clinic setting. As a consequence, medical and mental health leadership struggle to train and manage their staff to ensure that these challenging rounds are done in a way that finds patients who are in a worsening condition. Therefore, it is imperative that the staff doing the round have easy access to pertinent patient health information so they can prioritize their time with patients and maintain a better sense of which patients need to come out of their cells for further examination. Given the need to identify progressive worsening of patients that may go undetected from shift to shift, the EHR can also help by providing a means to track data over time. Currently, CHS is designing a solitary confinement template that staff can use with a tablet computer. A key feature of this template will be to prompt collection of objective data on each patient during rounds. For example, providers are prompted to enter whether a patient has taken their medications, engaged with the staff, or been out of their cell for their allotted services. This leads to a daily report that indicates which patients appear to be faring poorly and should be removed from these settings.
This type of template can also be used in non-solitary confinement settings. For example, approximately 800 patients reside in mental health units, where mental health staff must conduct daily rounds. These rounds are in addition to weekly individual encounters and daily group sessions, and they exist to help staff know when patients need a higher level of care. These units are chaotic, sometimes violent settings where staff may lose track of patients who are quietly decompensating. A daily round template is being designed to capture objective variables that will allow for the provider to have a relatively quick encounter, but also generate a daily report of patients who should be evaluated for hospital transfer.
In addition to creating structured templates that capture data from the clinical encounter, the EHR has been modified to capture a broad array of reasons to explain patients missing their clinic appointments. Patient production is a vexing issue for all correctional health providers. Patients with mental illness are often at a disadvantage in accessing health care, either by dint of competition among types of appointments or because specialized housing settings may actually create barriers to receiving care or services outside the unit. Patients in these settings often require dedicated security escort to leave their units, and lack of escort is a common reason for poor patient production. In addition, patients in mental health units are at higher risk of being injured during their incarceration and they may be reluctant to risk encounters while venturing out of mental health units. Accordingly, a variety of codes exist in the EHR so that when patients do not attend their appointments, a reason can be entered, such as ‘no escort available’ or ‘patient refused.’ Health staff share these reports with security staff and leadership to improve patient access to care.
The connection of the jail-based EHR to a state-wide health information exchange (HIE) might serve as one key development that will further promote the human rights of CHS patients. The HIE represents a repository into which all health systems may enter key health information and from which providers can access information about the care their patients have received. The unit of exchange in the HIE is known as the continuity of care document (CCD). The CCD is a medical summary that all EHRs can produce and is designed to allow for exchange of important information such as medications, problem lists, and laboratory results across health systems. This stands to improve the care that patients receive while in jail by assisting clinical decision-making for providers. For example, patients who arrive in jail and cannot recall complicated regimens of medications will be able to provide consent to their providers, allowing access to their community records. Conversely, community care providers will know what care their patients received while in jail. Injuries, mental health exacerbations associated with solitary confinement, and other known health risks of incarceration will become more transparent for individual providers, health systems, and plans that pay for care. Our hope is that these entities may translate their newfound information and financial stake in these outcomes into pressure for improved conditions of confinement and reduction in reliance on incarceration. Because correctional health settings are increasingly adopting EHRs, the adaptation of the EHR to promote human rights will not incur significant extra cost. Most EHRs are highly adaptable and limited only by the interest of the health leadership in adapting treatment to allow for surveillance of vulnerable populations.
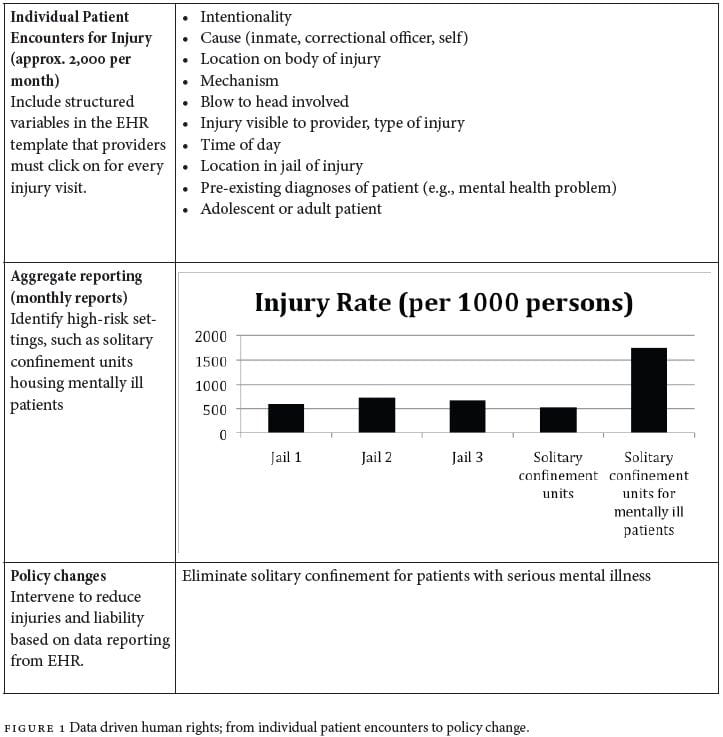
Although most benefits of EHR adoption are seen in provision of individual care and surveillance of vulnerable populations, there is a clear and important role for the EHR in providing data to state actors, such as municipal and state governments who oversee correctional settings, and who carry duties to ensure prisoners’ human rights are not violated. Transparency is one of the most critical yet elusive aspects of administering correctional settings. In extreme cases, one state actor may infiltrate correctional settings in order to investigate the actions of another.10 The EHR allows for the health service to not only maintain focus on core human rights concerns within a correctional setting, but for state actors to also maintain better surveillance on the health and well-being of the incarcerated. To the extent that reporting key data becomes automatic and routine, state actors can spend less time assessing the veracity of information and focus more quickly on addressing concerns. These data can then be used to promote policy changes that meet the needs and rights of patients, jail administrators, and state actors (see Figure 1).
Summary
Implementing the EHR in the NYC jail system represents a significant improvement in the ability of CHS to monitor and safeguard the human rights of patients. Three key elements of the EHR contribute to this improvement. First, the EHR can be readily altered to gather information related to abuse, neglect, or other human rights concerns. Second, the EHR allows generation of reports based on patient profile, time, location, or clinical outcome. Third, the EHR can be linked to outside EHRs through HIE so that injuries, mental health exacerbations, and other concerns unique to the correctional setting can be followed up in the community.
The connection of our EHR to the HIE will require significant educational collaboration with community health providers around the key pieces of information that may indicate jail-based vulnerability. In addition, our current EHR development priorities focus on using structured templates for cell side rounds in solitary confinement settings, and similar templates in mental health units. These templates will allow leadership in each jail to quickly know which patients should be removed (or precluded) from solitary confinement, or who need hospital transfer.
These human rights applications of the EHR represent the immediate human rights concerns for our clinical mission. Our approach has been to identify vulnerable groups of patients (e.g., the injured, those with mental illness) or those in high-risk settings (e.g., solitary confinement) and then adapt the EHR to improve care and monitoring for these patients. A broader set of concerns, including the right to access one’s own health information, the right to confidentiality, and the right to autonomy, is also important in further developing the EHR. Patients in jail often avoid care because they fear their information will not be confidential. This fear of engagement also contributes to patients not knowing or learning about their health problems, which are important features of autonomy. As we train our staff about human rights concerns, we plan to broaden the human rights applications that we build into the EHR, as well as increase patient participation in the process. Overall, the EHR has allowed us to promote human rights by identifying vulnerable populations and reporting on adverse outcomes associated with their vulnerability. In addition, this capacity for data aggregation and reporting has allowed us to start the implementation of policies that mitigate some of these vulnerabilities.
Sarah Glowa-Kollisch, MPH, is the Director of Policy and Evaluation in the Bureau of Correctional Health Services at the New York City Department of Health and Mental Hygiene.
Kelly Andrade, MA, is the Development Specialist in the Bureau of HCAI Information Technology and Initiatives at the New York City Department of Health and Mental Hygiene.
Richard Stazesky is the Assistant Commissioner of the Bureau of HCAI Information Technology and Initiatives at the New York City Department of Health and Mental Hygiene.
Paul Teixeira, DrPH, MA, is the Director of Program Support and Evaluation in Transitional Health Care Coordination, Bureau of Correctional Health Services at the New York City Department of Healthand Mental Hygiene.
Fatos Kaba, MA, is the Program Evaluator in the Bureau of Correctional Health Services at the New York City Department of Health and Mental Hygiene.
Ross Macdonald, MD, is the Medical Director of the Bureau of Correctional Health Services at the New York City Department of Health and Mental Hygiene.
Zachary Rosner, MD, is the Deputy Medical Director of the Bureau of Correctional Health Services at the New York City Department of Health and Mental Hygiene.
Daniel Selling, PsyD, is Executive Director of Mental Health in the Bureau of Correctional Health Services at the New York City Department of Health and Mental Hygiene.
Amanda Parsons, MD, MBA, is the Deputy Commissioner of the Division of Health Care Access and Improvement, at the New York City Department of Health and Mental Hygiene.
Homer Venters, MD, MS, is the Assistant Commissioner of the Bureau of Correctional Health Services at the New York City Department of Health and Mental Hygiene.
Please address correspondence to the authors c/o Homer Venters, 42-09 28th St, 10th floor, Queens, NY, 11101-4132. Email: hventer1@health.nyc.gov.
References
1. I. Binswanger, P. Krueger, and J. Steiner, “Prevalence of chronic medical conditions among jail and prison inmates in the USA compared with the generation population,” Journal of Epidemiology and Community Health 63/11 (2009), pp. 912-919.
2. T. Minton, Jail inmates at midyear 2011 – statistical tables (Washington, DC: U.S. Department of Justice, Bureau of Justice Statistics, April 2012). Available at http://www.bjs.gov/content/pub/pdf/jim11st.pdf.
3. J. Holroyd-Leduc et al., “The impact of the electronic medical record on structure, process, and outcomes within primary care: A systematic review of the evidence,” Journal of the American Medical Informatics Association 18/6 (2011), pp. 732-737.
4. P. Fontaine et al., “Systematic review of health information exchange in primary care practices,” Journal of the American Board of Family Medicine 23/5 (2010), pp. 655-670.
5. R. Stazesky, J. Hughes, and H. Venters, Implementation of an electronic health record in the New York City jail system (New York: New York City Department of Health and Mental Hygiene, April 2012). Available at http://www.cochs.org/files/hieconf/implementation-ecw-new-york.pdf.
6. R. Macdonald, A. Parsons, and H. Venters, “The triple aims of correctional health: Patient safety, population health, and human rights,” Journal of Health Care for the Poor and Underserved 24/3 (2013), pp. 1226-1234.
7. A. Ludwig et al., “Injury surveillance in New York City jails,” American Journal of Public Health 102/6 (2012), pp. 1108-1111.
8. F. Kaba et al., “Traumatic brain injury among newly admitted adolescents in the New York City jail system,” Journal of Adolescent Health (2014), e-publication ahead of print.
9. F. Kaba et al., “Solitary confinement and risk of self-harm among jail inmates,” American Journal of Public Health 104/3 (2014), pp. 442-448.
10. D. Ono, “Further indictments forthcoming in federal investigation of LA County jails?” ABC 7 News (January 24, 2014). Available at http://abclocal.go.com/kabc/story?id=9406856.