“Small places close to home”: Toward a health and human rights strategy for the US
Elizabeth Tobin Tyler
Health and Human Rights 15/2
Published December 2013
Where, after all, do universal human rights begin? In small places close to home.
–Eleanor Roosevelt
Abstract
Much of the discussion about “health as a human right” has centered on global health initiatives, largely ignoring the application of human rights principles to the significant socioeconomic and racial health disparities in the United States. Given the persistent gaps in insurance coverage and access to quality preventive care in the US, the health and human rights movement has primarily focused its efforts on achieving universal health care coverage. However, this focus has left unaddressed how a human rights strategy might also address the social determinants of health. As Americans’ health continues to worsen—the US Institute of Medicine recently reported that the US now fares worse in nine areas of health than 16 peer high-income democracies—a broader social determinants approach is warranted. This article explores the application of international human rights principles, including a “right to health” to the US context, and analyzes how existing domestic law may be used to advance health as a human right for America’s most vulnerable populations. It demonstrates that an effective health and human rights strategy must build partnerships among health care providers, public health professionals, and lawyers to identify rights violations, hold officials and systems accountable, and mobilize communities to advocate for systems and policy change.
Introduction
In 1996, Jonathan Mann, former director of the Global Program on AIDS at the World Health Organization, lamented the “lack of a coherent conceptual framework for analyzing societal factors that are relevant to health.” He worried that “[p]ublic health action based on social class is often simply accusatory, and it raises, but cannot answer, the question: ‘what must be done?’ In this sense, ‘poverty’ as a root cause of ill health is both evident and paralysing to further thought and action.”1 He concluded that a human rights framework was the most “useful approach” for responding to the social determinants of health.2 Scholarship and activism arguing for a human rights approach to “the right to health” have been particularly prevalent in the past two decades as research has continued to document the role of social determinants in poor health outcomes and health inequity around the world.3
Yet much of the discussion of health and human rights has centered on global health initiatives, mostly ignoring the application of human rights principles to the United States. Discussion of “health as a human right” in the US has focused primarily on the movement for universal health care coverage. This is hardly surprising given the enormous inequities in access to care that continue to plague the US. The Patient Protection and Affordable Care Act of 2010 (PPACA, henceforth ACA), while significantly expanding coverage to the uninsured, will not end the debate in America about the need for the realization of the right to health care.
Nonetheless, the focus on health care has left unaddressed how a human rights strategy might also address the role of the social determinants of health in creating health disparities in the US. Recent studies indicate that US health outcomes continue to worsen in comparison to other wealthy nations. The US Institute of Medicine recently reported that the US now fares worse in nine areas of health than 16 peer high-income democracies.4 Another study found that while overall population health in the US improved from 1990 to 2010, “[m]orbidity and chronic disability now account for nearly half of the health burden in the United States”5…and “[i]mprovements in population health in the United States have not kept pace with advances in population health in other wealthy nations.”6 Recent literature also points to the well-documented social gradient in health in the US that runs the spectrum from those at the top to those of the bottom of the income scale.7 Understanding how social factors, such as income level and social status, contribute to worsening morbidity, disability, and chronic disease in the US and how these factors lead to health disparities across groups is fundamental to improving the public’s health.
This article explores the application of human rights principles, including the right to health to the US context. In order to answer Mann’s fundamental question, “What must be done?” to respond to poverty as a root cause of illness, it is important to explore not only the application of international human rights law, but also how existing domestic law may be used to advance health as a human right for America’s most vulnerable populations.
The article begins with a discussion of international human rights laws that promote the right to health, followed by an analysis of their potential for guiding a health and human rights agenda in the US. It then explores the potential for developing a multilevel strategy for framing a right to health in the US. Components of such a strategy could feature the use of international human rights principles to frame national health policy, state constitutional and legislative efforts based on human rights law, and finally, the enforcement and strengthening of existing laws that protect and promote the health of vulnerable populations. To successfully frame a health and human rights strategy in the US, it is essential that the health care, public health, and legal communities unite to effect change at the community as well as the state and national levels.
The human right to health
Human rights are understood to be rights afforded to all people by virtue of the fact that they are human beings.8 Human rights are recognized principles or norms that apply to all people, regardless of where they live or their status in a given society. As a declaration of universal principles, the concept of human rights represents an aspirational vision of a just society. International human rights law embodied in the Universal Declaration of Human Rights (UDHR), the International Covenant on Civil and Political Rights (ICCPR), and the International Covenant on Economic, Social and Cultural Rights (ICESCR), together deemed the “International Bill of Human Rights,” articulate human rights standards for every individual. This international body of law not only addresses political and civil rights, but also articulates particular social and economic rights needed to realize an individual’s human potential. Article 25 of the UDHR, for example, states:
Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing, and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control.9
Article 25 explicitly recognizes that health and well-being are inextricably tied to the social conditions in which people live, the opportunities that they have, and the distribution of resources in their community.10 In interpreting this right, the question of what standard of living is “adequate” to protect health and well-being is complex. As will be discussed later, this question is particularly relevant for any discussion of the human right to health in the US where there is strong disagreement about whether or not all citizens enjoy, or at least have access to, an “adequate” standard of living for health.
Similarly, there has been criticism of the “right of everyone to the enjoyment of the highest attainable standard of physical and mental health” as articulated in Article 12 of the ICESCR as vague and difficult to enforce.11 Despite efforts by the Committee on Economic, Social and Cultural Rights to further define the right in General Comment 14 adopted in 2000 to include health care, education, and other underlying social determinants of health, “one is hard pressed to find a more controversial or nebulous human right than the ‘right to health.’” 12,13
Yet, recent research about and attention to the role of social determinants in individual and population health have spurred new dialogue among public health officials, lawyers, and scholars about the importance of defining the human right to health as a mechanism for holding governments accountable and for developing responsive policy.14 The complex relationship between the social determinants of health and human rights is perhaps best understood in this way: social determinants, such as access to the provision of food, safe housing, education, and work are “both human rights themselves and are necessary for health.”15
The WHO Commission on the Social Determinants of Health (SDH) has embraced a human rights framework as fundamental to realizing health equity. In pronouncing that “[t]he international human rights framework is the appropriate conceptual and legal structure within which to advance towards health equity through action on SDH,” the WHO Commission raises a fundamental question about the distinction between broad aspirational human rights principles (such as “the right to the highest attainable standard of health”) and enforceable individual legal rights.16 Scott Burris points out the importance of delineating “human rights” and “human rights law”:
…[t]he former term referring to the universal entitlements of human beings to certain opportunities and immunities, and the latter to the evolving body of international and state law more or less effectively embodying and implementing these rights. On this view, “law” is a somewhat narrower concept than human rights, at best an instrument of its fulfillment, at worst a violation of human rights, and in many instances simply irrelevant.17
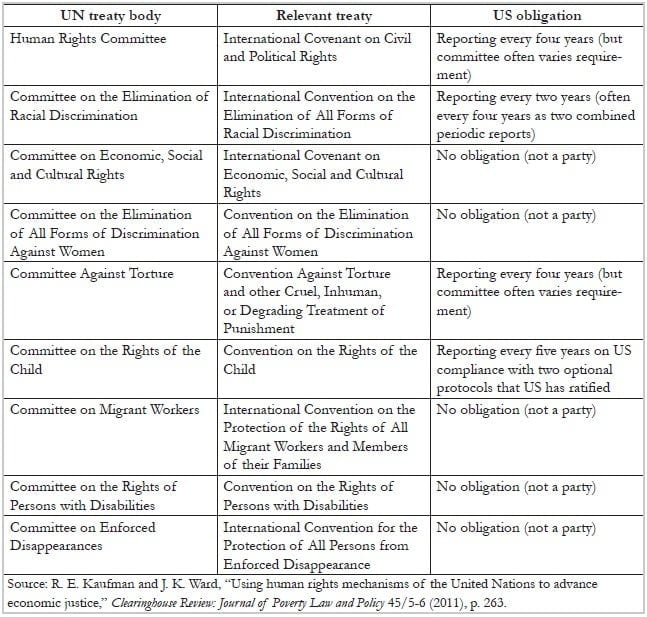
This distinction is particularly important for any discussion of human rights or the right to health in the US, since it is a signatory but not a party to the ICESCR. Table 1 shows international human rights treaty bodies and US obligations under them. Even for party states, the legal obligation for the state to “respect, protect and fulfill” the right to health in its own borders is couched in the idea of the “progressive realization,” rendering it difficult to determine when a state has breached its obligation.18 While international human rights laws articulate a shared value about the right to health, a value that the US claims to endorse, it is important to evaluate what role these laws, if any, can play in advancing health equity in the US, without the teeth of enforcement.
Table 1. International human rights treaty bodies and US obligations
Human rights in the US
The recent history of US engagement in international human rights represents a relinquishment of the leadership role Americans once had in bringing nations together to establish universal human rights principles, including positive social and economic rights. Despite US leadership in drafting the UDHR after World War II, the political and social context of the postwar years led to a focus on civil and political rights and an abandonment of the promotion of social and economic rights. Scholars have cited three historical developments as critical here: the geopolitical divide created by the Cold War, the rise of American exceptionalism, and the fierce opposition to scrutiny of legalized racial discrimination in the US during the Jim Crow era against international human rights standards. 19,20 While it is beyond the scope of this article to detail the history of human rights policy in the US, understanding these historical foundations is critical to the discussion of a right to health in the US.
Additionally, the US refusal to ratify the ICESCR and past concerns raised by US officials about government accountability for economic, social, and cultural rights is instructive in understanding the current US position. First, the US has raised the possibility that ICESR could create an “internationalization of responsibility” by Western countries for ensuring that social and economic rights were met in underdeveloped countries. Second, US officials have repeatedly insisted that making social and economic rights justiciable would create “the basis for an individual legal cause of action against the government by persons who differ with that government’s policy approaches or priorities.”21 Human rights scholars have refuted both of these concerns.22 Nonetheless, these concerns illuminate the resistance in the US to move the human rights agenda beyond aspirational statements either internationally or domestically. Indeed, the underlying fear is “that the legal recognition of economic and social rights in the US might lead to fundamental changes in the socioeconomic order.”23
The US focus on political and civil rights at the expense of social and economic rights has continued to disappoint human rights advocates in the US. For example, the US government report to the United Nations Human Rights Council submitted in 2010 as part of the first-ever Universal Periodic Review process once again “sidestepped any obligation to implement any economic and social rights.”24 However, many felt that the Council’s outcomes report was a significant step forward in documenting US failures with regard to social and economic rights.25 Of note, many of the 228 recommendations of the Council to the US concerned social rights, including the right to adequate housing and health care.26
Framing a right to health in the US
The right to health care
Exploring the right to health in the US as it relates to social determinants of health requires first addressing the lack of a right to health care coverage. The US is the only industrialized nation in the world without a plan providing universal health care coverage and a legal recognition of the right to care.27 There is no constitutional right to health care and the federal statutory rights to health care coverage for the poor, elderly, and disabled (Medicare and Medicaid) are limited to those who are deemed “deserving” and are far from universal.28 Because eligibility is categorical (based on a particular status—age, disability, or income level), these programs are premised on the notion that health care coverage should be provided by the government only when an individual deserves help—for example, because she or he is elderly, disabled, or poor—not because government should afford coverage to all citizens as a right.
Even with passage of the ACA, followed by the US Supreme Court decision upholding the law’s provisions, Americans’ health care rights will remain “inherently unstable,” in the words of David Orentlicher.29 By choosing an approach which favors expansion of the market-based health insurance system over universal coverage, failing to fully address the existing problems with access to health care for the underserved, and with the Supreme Court’s decision in National Federation of Independent Business v. Sebelius, essentially delegating many of the eligibility standards for Medicaid to the states, the ACA will still leave many out of the health care system.30 It is estimated that there will continue to be 30 million uninsured non-elderly adults into the next decade.31
While the ACA is a significant step forward in expanding health insurance coverage and offering federal oversight and funding to improve health care quality and efficiency, the failure to extend universal and uniform coverage means that the US still falls far short of fulfilling a human right to health care. In fact, by remaining a market-based health care system, the US continues to treat “health care as a market commodity to be bought and sold for profit rather than as a human right.”32 Nonetheless, as will be discussed later, some of the ACA’s provisions may offer important opportunities and resources for states and localities to address the social determinants of health.
Social determinants and the right to health
While much of the initial literature on social determinants focused on global health, attention to the role of poverty, race, and social marginalization in US health disparities has spurred significant recent research, policy discussion, and investment by foundations such as the Robert Wood Johnson Foundation.33 Although causal pathways between social determinants of health and poor health outcomes can be complex to tease out, social epidemiological research leaves no doubt that social environment affects individual and population health.34
The recent research showing the links between social conditions and health outcomes helps to reinforce the human rights concept of a right to health as opposed to a right to health care. Health inequity, which Paula Braveman defines as “health differences that are systematically linked with social disadvantage and that entail worse health among disadvantaged groups,” are “particularly relevant to social justice and to human rights because they may arise from intentional or unintentional discrimination or marginalization and, in any case, are likely to reinforce social disadvantage and vulnerability.”35
Understanding the role of law in constructing and reinforcing social conditions that affect health is also critical to defining a human right to health. Recent public health law research has illuminated the role of law in constructing the environments in which people stay healthy or get sick.36 Importantly, it points to how local, state, and federal laws and policies—and their implementation through a system of rules and practices—bear on the health of individuals and communities.37
At the core of health inequity in the US are the political and social systems which drive socioeconomic status and income inequality. Delineating what kinds of social conditions equate with the definition of “poverty” or “extreme poverty” in the US is a controversial matter, as are perceptions about the underlying causes of poverty and marginalization. 38,39 Americans appear to be almost evenly split between attributing poverty to “circumstances beyond [people’s] control” (45%) and those viewing poverty as the result of individuals “not doing enough to help themselves” (48%).40 Because of differences in perspectives on the roots and definitions of poverty, there is strong resistance to the idea of comparing deprivation in the US to other countries, particularly underdeveloped countries. Nonetheless, “[h]uman rights advocacy is informed by a recognition that individuals and groups in the United States also suffer human rights violations comparable to violations abroad, thus avoiding the ‘our culture and theirs’ bifurcation.”41
A 2012 report by the National Poverty Center calculated the number of US households with children living in extreme poverty. Adapting one of the World Bank’s main indicators of global poverty, the study defined households to be in extreme poverty “if they report [living on] $2 dollars or less per person, per day in total household income in a given month (approximated as $60 per person, per month in 2011 dollars)” and found that in 2011, 1.46 million US households with 2.8 million children met this definition, a 129% increase from 1996. When SNAP benefits (food stamps) were counted as income, 800,000 households and 1.4 million children still met this definition of extreme poverty.42 Through a human rights lens, the level of deprivation existing among these Americans can be interpreted as the state’s failure to ensure its citizens a sufficient standard of living adequate for health and well-being. Yet in a 2007 survey by the Opportunity Agenda, only 52% of Americans said that freedom from extreme poverty should be considered a human right.43 Interestingly, 72% of those polled believed that health care should be considered a human right.44
The American tendency to attribute poverty and low social status to individual failure makes advocacy efforts focused on legal rights or policy failures difficult. A 2004 Ford Foundation report documenting human rights advocacy in the US highlights the enormous resistance encountered by advocates who characterize their work as based on human rights.45 A pragmatic fear of dismissal from policymakers and courts has kept lawyers concerned with social and economic rights from exploring broader human rights claims. Hence, legal advocacy focused on access to food, housing, education, and health care has remained primarily focused on addressing one issue at a time rather than as part of a wider human rights strategy linking economic and social rights.46
Legal and policy discourse has tended to blame poor health in America on an inefficient health care system, individual health choices, and budget cuts. This has silenced community critique. However, framing US poverty, deprivation, and health inequality in terms of the interdependence of economic and social rights can invigorate community-level activism. Including those affected by the social determinants of poor health in the discussion is not enough. Those who are affected must generate the agenda for an effective human rights advocacy strategy through a community-based approach that rejects lawyer-driven litigation as the primary tool in effecting change.47
Hence, as the following section describes, promoting the right to health in the US must not solely depend on international human rights law arguments in US courts; rather, a human rights strategy must include efforts close to home, which challenge US social and legal policies that permit the violation of economic and social human rights.
Toward a health and human rights strategy for the US
While, as noted above, American lawyers and other advocates have encountered strong resistance when they have defined their efforts as human rights work, several factors point to momentum for a health and human rights strategy in the US.
First, with the growing attention to the social determinants of health and the need for a global health and human rights framework, it would be illogical (and would completely bow to the idea of American exceptionalism) to exclude the poor health outcomes and entrenched socioeconomic and racial health disparities in the US from this dialogue. Second, the ACA, despite its expansions and reforms, will not offer a panacea to the health care crisis in the US. Recent studies document that income gradients in health have persisted despite universal health care coverage in the UK.48 This persistence illustrates the significance of social and economic factors in health and the need for a broader strategy to address health disparities.
In recent years, US organizations concerned with health and human rights have begun to apply human rights principles to the US. The following sections first explore how some recent trends in federal and state courts’ use of international human rights law may offer an opportunity for advocates to make health and human rights arguments. Second, they consider how state constitutions, which often provide greater protections for social and economic rights, may provide an opening for arguments about the right to health. Third, they argue that US legal services for the poor should be reframed around a human rights strategy that acknowledges the interdependence of social and economic rights and health while applying a multilevel community-based legal and policy advocacy strategy. Finally, the paper contends that utilizing community-based data and building partnerships among public health advocates, health care providers, and lawyers are the most effective means to build opportunities for community legal empowerment and for social accountability.49
Applying international human rights standards in US courts
Recent Supreme Court decisions acknowledging international human rights norms have raised hopes among human rights advocates that these arguments may be gaining traction in domestic courts.50 While the Supreme Court has been careful to assert that use of international human rights law in its decisions is not dispositive, and the cases where the court has cited international law principles have focused on civil rights, not social or economic rights, there is reason to be encouraged. The Court’s willingness to acknowledge arguments based on international law opens a small window for application of human rights law in the US. It is important to point out, however, that lawyers are turning to international human rights law for support, in part, because of the narrowing of civil rights and constitutional protections in the US over the past decade.51 Arguments based on human rights principles interpreting the US Constitution have rarely succeeded, and have never succeeded with regard to positive social and economic rights.
Constitutional arguments
While some countries, most notably South Africa, have incorporated social, economic, and cultural rights in their constitutions, the US Constitution has repeatedly been interpreted not to afford any positive social or economic rights. Poverty lawyers’ efforts over the years to challenge federal and state practices that fail to ensure a basic standard of living have mostly fallen on deaf ears. 52,53 Particularly with regard to social and economic rights, US courts express concern that judicial enforcement will always require the court to wade deep into policymaking more appropriate for the legislative branch.54
Yet, lawyers are increasingly applying human rights arguments in state cases where courts have the authority to consider international law in interpreting state statutory and constitutional provisions.55 In fact, as Martha Davis points out, state courts not only have the authority to implement international law, they have the obligation to do so under the Supremacy Clause of the US Constitution: “[A]cceptance of the federal constitution and its provisions regarding treaties is an obligatory undertaking upon acquiring statehood, regardless of the text of the state’s own constitution. This undertaking requires states to honor the federal government’s treaty responsibilities. Nevertheless, some state actors seem oblivious to their constitutional obligations.”56
Furthermore, because many state constitutions include provisions recognizing social and economic rights based upon or similar to language in international human rights law, and are “often more malleable”57 than the federal constitution, they offer opportunities to challenge state action (or inaction).58 Most relevant to the discussion of health and human rights is Article XVII of the New York State Constitution which imposes an affirmative duty on the state to address the health of its inhabitants: “The protection and promotion of the health of the inhabitants of the state are matters of public concern and provision therefor shall be made by the state and by such of its subdivisions and in such manner and by such means as the legislature shall from time to time determine.”59 Article XVII, Section 1, which recognizes that “the aid, care and support of the needy are public concerns and shall be provided by the state,” could be used to frame a strategy on social determinants of health and human rights, based on the state’s obligation to provide for the health and well-being of its citizens.60
Additionally, according to some analysts, the growing body of international law interpreting the enforceability of social and economic rights, particularly recent holdings of the South African Constitutional Court, may provide useful guidance for US courts, including state courts.61 The South African court’s decisions in Republic of South Africa v. Grootboom (interpreting the state’s obligations with regard to the right to housing) and Minister of Health v. Treatment Action Campaign (interpreting the state’s responsibility to undertake reasonable measures to ensure access to health care) provide examples of the justiciability of constitutional protections for social and economic rights. While state courts have yet to impose an affirmative governmental duty to enforce a state constitutional provision asserting a right to health, the willingness of some courts to look abroad for guidance may offer some key opportunities.
New state legislation incorporating human rights principles
Vermont’s passage in 2011 of “An Act Relating to a Universal and Unified Health System” was the result of a grassroots campaign by the Vermont Workers’ Center to frame health care as a human right. The campaign brought together a wide range of constituents, including business, labor unions, community organizations, health care providers, and lawyers to lobby for a universal, publicly-financed, and equitable health care system in the state.62 Furthermore, using human rights principles, advocates averted a proposed amendment to the legislation that would have prevented undocumented immigrants from participating in the system.63 The campaign “was conceived as a vehicle for building a broad-based movement for social change, encompassing a social and economic justice agenda beyond the single issue of universal health care.”64
Of course, a state-by-state approach to human rights represents a slow and incremental approach to a human rights advocacy agenda for the US. Nonetheless, as is evident from the marriage equality movement, state actions can serve to inspire change in other states; once one state takes a chance, other states often follow suit. A state constitutional or legislative strategy is only one aspect of a health and human rights strategy. Reframing the role of lawyers and legal aid programs in the US to move beyond single issue advocacy and to explicitly address the social determinants of health using law as remedy is also a critically important health and human rights approach.
Reframing US legal aid as health and human rights advocacy
Reframing one’s work in human rights terms takes you back to the primacy of equality and dignity no matter what the circumstance. Once you reassert that basic principle, peoples’ perceptions of the problem change and new avenues for advocacy open up.65
A number of recent articles discuss the limitations of traditional legal aid programs to bring about systemic changes in the areas of social and economic rights.66 One of the main critiques of traditional legal aid programs is that they “tend to structure their efforts according to the problems that clients bring forward,” rather than develop a broad-based strategy for protecting and promoting social and economic rights.67 They also continue to offer top-down services at the expense of engaging the communities they serve:
[T]he isolation of legal services organizations from the communities they serve often perpetuates the top-down service delivery model. In addition, a legal services organization’s focus on professionalism, together with limitations on the types of legal practice permitted under funding rules and the lack of a clear, comprehensive vision for productive community involvement, has channeled much of the work of legal services lawyers into the courts instead of the communities.68
Another critique is the dichotomization in many legal programs between individual representation versus impact litigation aimed at advancing the interests of multiple clients through systems reform.69 Due to federal restrictions many legal aid programs no longer engage in class action litigation or legislative advocacy.70 US poverty lawyers have begun to challenge this dichotomy, suggesting that a community-lawyering approach that applies multiple advocacy strategies, including litigation and policy change, in partnership with the client community is most effective.71 In terms of a human rights strategy to advance social and economic rights, a key component of advocacy is educating people in a given community about their rights, human rights principles, and the potential for using law as a tool to promote those rights.72
Health and human rights advocacy close to home
Though critically important, the federal government is “just one out of the complexity of the nearly 88,000 governments in the United States federal system.”73 Local and state governments provide and administer social and economic goods and services. Many human rights abuses in the US occur due to daily indignities experienced by vulnerable people in their interactions with unresponsive systems. Often, these daily struggles follow from the failure to enforce laws intended to provide a safety net, safe and habitable housing, an adequate education, and protection from violence for poor and disenfranchised people. Federal, state, and local laws and regulations governing the distribution of basic needs may not be adequate, but access to justice in the US also plays a large role in what can be described as social and economic human rights issues.
Moving beyond traditional legal aid approaches focused on crisis-driven litigation, a multifaceted community-based advocacy strategy must map where, when, and why enforcement failures occur and hold government actors accountable. As Vivek Maru has eloquently pointed out, enforcing human rights in the US, as elsewhere, is not just about changing or strengthening laws, it is also about enforcement:
Some law scholars and human rights organizations have held that spheres like health and education are matters of political process, not rights. But whether or not a polity grants abstract fundamental rights to social and economic goods, any health or education or housing policy inevitably creates specific entitlements and, in turn, a chain of responsibility to ensure that those entitlements are fulfilled. Legal empowerment programs strive to understand that chain of responsibility, no matter how faulty, and to get it to work for people.74
One of the dangers of focusing a health and human rights strategy solely on international law or litigation is that of losing sight of the differential enforcement of existing laws and policies experienced in neighborhoods and communities every day. Failure to enforce housing standards, restraining orders, Individual Education Plans, workplace protections, as well as rights to public benefits and health care, are the “bread and butter” issues affecting the standard of living, opportunities, and health of vulnerable people.75 But clearly a strategy of case-by-case advocacy is also insufficient as a health and human rights agenda.76 The ultimate goal is systems accountability and change. This will only come with lawyers and health care providers partnering with and empowering communities to enforce and articulate their rights as human rights.
Joining legal empowerment and social accountability
Maru argues that a human rights strategy should join legal empowerment and social accountability:
Legal empowerment efforts grow out of the tradition of legal aid for the poor; they assist citizens in seeking remedies to breaches of rights. Social accountability interventions employ information and participation to demand fairer, more effective public services. The two approaches share a focus on the interface between communities and local institutions.77
While Maru is speaking to the international human rights context, his argument is equally applicable to the US. Human rights advocacy depends on a range of strategies, including community legal education, fact-finding, documentation, and media campaigns, as well as litigation and legislative advocacy to promote more sustainable systems changes.78 As some legal aid programs move toward a more holistic, community-lawyering approach, the time is ripe for shifting focus to legal empowerment based on human rights advocacy tactics.79 But what has also been missing from much legal aid work in the US is “social accountability practitioners’ use of aggregate data as a catalyst for community action.”80 Public health law research represents an important example of social accountability through methodologies that collect data about the health effects of particular laws and policies. The goal of this research is to effectively connect data to community-based advocacy strategies through partnerships between lawyers and public health practitioners. Linking these efforts to community mobilization and advocacy efforts will be a critical next step for this approach.
A systemic health and human rights strategy should be built upon interdisciplinary partnerships among health care providers, public health practitioners, lawyers, and community organizers. It should be founded on three principles: bearing witness to human rights violations within the community context; tracking systemic failures through data collection and monitoring; and broad-based legal strategies which include both individual and policy advocacy in a given community. This type of partnership is explored below.
Partnerships among health care, public health, and law professionals
Because health care providers bear witness daily to what might be defined as human rights abuses in the US—homelessness, childhood hunger, the failure of the government to protect victims from domestic violence—they are indispensable in articulating how these violations impact the right to health. “Health workers have long acknowledged the societal roots of health status; the human rights linkage may help professionals engage in specific and concrete ways with the full range of those working to promote and protect human rights and dignity in each society.”81 Health care providers concerned with human rights often experience enormous frustration in their own inability to remedy their patients’ poor social conditions. Health care workers who practice in low-income communities often see an unrelenting flood of patients who go without basic services. Enforcement of legal rights is beyond the scope of their practice; to advocate effectively for their patients’ basic needs, therefore, they need to partner with community and legal advocates. Nonetheless, their voices are critical in documenting human rights violations and advocating for policies that secure basic human needs.
Public health practitioners are expert at data collection and systems monitoring. But often data are not fully utilized for social accountability, particularly at the community level. Data collection may also not target the government systems and structures that impact health but are outside the realm of more traditional public health policies. For example, government systems which unlawfully deny access to government benefits or health care, fail to enforce housing codes, or deny a homeless child school entry, all affect health. As Maru points out, those attempting to document systems failures in relation to health should be aware of how the legal framework shapes those systems and the potential for legal advocacy:
Social accountability practitioners may tend to ignore this broader legal framework because of the perception—often valid—that the law and state structures are largely unresponsive and dysfunctional. But legal empowerment practitioners specialize in squeezing justice out of dysfunctional systems.82
Both quantitative and qualitative studies that monitor population health outcomes and systems delivery (within the health care sector and outside of it) are needed to carry out a health and human rights strategy that targets social determinants. Health care providers’ voices are critical to data collection.
As Maru writes above, lawyers are trained to “squeeze justice out of dysfunctional systems.” Working in partnership with health care providers and public health practitioners, they can effectively build an arsenal of evidence to challenge the systems which deny basic human rights. In partnership with health care providers, they can use a range of advocacy strategies on behalf of individual clients who are denied justice through failure to enforce their legal rights. They can work directly with health care providers to document abuses and advocate for systems changes. With the help of public health practitioners and health care providers, lawyers can collect and use data to document systemic failures.
Finally, lawyers, health care providers, and public health practitioners can work together with affected communities to mobilize advocacy efforts drawing on principles of human rights and dignity that are often lacking from single-issue campaigns.
Medical-legal partnership as a human rights strategy
The medical-legal partnership (MLP) movement in the US exemplifies a community-based health and human rights strategy that implements a legal advocacy and social accountability approach by connecting lawyers, health care providers, and public health practitioners. The MLP model, first established in a safety-net hospital pediatrics department in 1993, now exists in over 500 legal and medical institutions in the US. The model is also being adopted in both Australia and Canada.
MLP is a healthcare delivery model that integrates legal assistance as a vital component of healthcare. Built on the understanding that the social, economic, and political context in which people live has a fundamental impact on health, that these social determinants of health are often manifested in the form of legal needs, and that attorneys have the special tools and skills to address these needs, MLP brings legal and healthcare teams together to provide high-quality, comprehensive care to patients who need it most.83
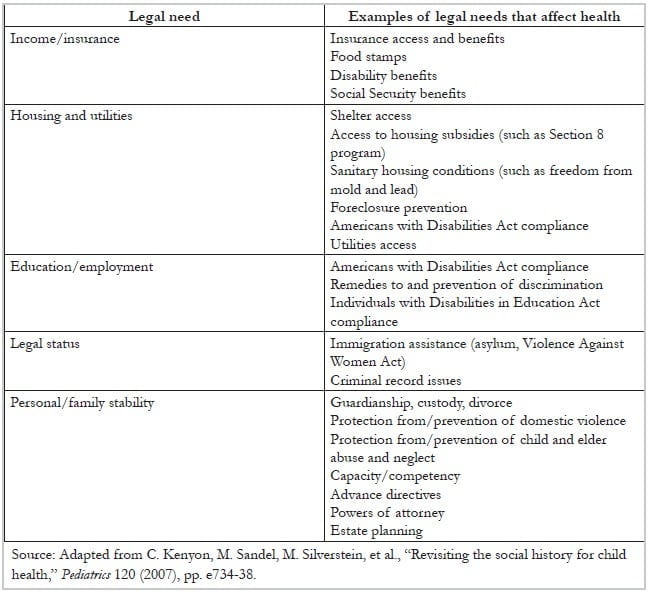
MLP reframes traditional legal services for low-income clients to specifically address the legal needs that implicate social determinants of health. Table 2 provides examples of legal needs that affect health. By defining legal rights based on access to basic human needs—income/insurance, housing and utilities, education and employment, legal status, and personal and family stability—MLP is a human rights approach to health.
Table 2. Legal needs that affect health
In “From Principle to Practice: Moving from Human Rights to Legal Rights to Ensure Child Health,” MLP pioneers Barry Zuckerman, Ellen Lawton, and Samantha Morton argue that legal advocacy focused on social determinants is critical to a health and human rights approach: “[A]s we continue to push for rights-based laws around the world, we also encourage an active strategy of promoting enforcement of existing laws….”84 Placing lawyers in community safety-net health care institutions in partnership with health care providers can result in early detection of rights violations. Hence, MLP is both preventive law and preventive medicine. It explicitly moves the enforcement of legal rights affecting health upstream by screening patients for social needs, thus identifying potential legal action before the patient/client is in crisis.
Importantly, MLP also extends far beyond enforcement of individual legal rights. In addition to reframing legal services to address social determinants, MLP transforms health care practice by training frontline health care providers to incorporate social and legal needs screening into their practice and to partner with lawyers to remedy these injustices. MLPs also create institutional structures which enable the tracking of rights violations and systemic failures affecting patient health outcomes in a given community. MLPs have successfully utilized data mapping to link poor community health outcomes with rights violations, thus incorporating public health strategies for addressing the social determinants of health.
A recent study by Beck and colleagues exemplifies how MLPs identify rights violations and lead to improved living conditions for a low-income community. 85 An initial MLP case involved a family with two children served by the Pediatric Primary Care Center (PPCC) at Cincinnati Children’s Hospital Medical Center. Both children had been diagnosed with asthma and one child was diagnosed with an elevated lead level. The family was referred to the MLP lawyers “after reporting pest infestation, peeling paint and water leakages during a visit for well-child care.” As additional housing conditions cases were referred, the MLP team identified a pattern of substandard housing conditions for a cluster of children living in units in six Cincinnati building complexes owned by one firm.
All of the affected children were African-American, were on public insurance, and had significantly higher rates of asthma, developmental delay, and lead poisoning than the general clinic population. In addition to litigation, MLP lawyers worked with the tenants association, met with city housing inspectors and planners, and appeared at city council meetings. Legal advocacy was not limited to housing conditions; it also included helping families with access to public benefits and enforcement of their children’s educational rights.86 As a result of MLP advocacy, 11 of the 19 building complexes with the same owner received significant repairs, impacting a larger community of tenants than the originally referred cases.87
The study authors concluded that:
Our MLP served as a mechanism for patient-level social and/or environmental risk identification and intervention, along with a parallel “diagnosis and treatment” of a community-level health risk. Such community-wide interventions can be difficult to fund and sustain. Rather than creating de novo services, the MLP model is more financially sustainable by focusing on enforcing existing ordinances and working with existing community agencies.88
MLP is a health and human rights strategy that employs the enforcement of existing legal protections in concert with community-level risk assessment and intervention to improve health. MLP is also a powerful tool for identifying the failure of existing laws and regulations to protect health and for bringing the daily experience of clinicians and patients to policy debates. Thus, “[a] unique advantage of MLP in the policy realm is the foregrounding of the clinical voice and perspective in debates regarding laws, rules, regulations, and practices—often allowing for strategies outside the traditional litigation model, and maintaining a critical focus on how policy will impact health and well-being.”89
Conclusion
While the US does not have a strong track record of applying international human rights principles within its own borders, particularly those that promote social and economic rights, recent developments—passage of the ACA, acknowledgment of international human rights laws by state and federal courts, and legislative achievements like that in Vermont explicitly defining health care as a human right—offer some hope that a human rights framework can advance a broader health and human rights movement. Recent studies documenting the declining health status of Americans as compared to other countries and the growing body of research demonstrating the significant role that social determinants play in poor health outcomes suggests that a broader health and human rights agenda is warranted.
In addition to promoting equitable access to health insurance and health care, a health and human rights agenda must include measures for combatting harmful social determinants and promoting environmental, economic, and social conditions beneficial to health. This type of advocacy necessarily evokes a discussion of the role of social and economic rights in health, such as individual and family economic stability, safe and affordable housing, equal access to educational opportunity, and freedom from domestic and community violence.
While advocates should continue to promote broad human rights principles at the state and federal levels in furtherance of better health outcomes, enormous strides can be made close to home by partnerships among health care providers, public health professionals, and lawyers to identify rights violations, hold officials and systems accountable, and advocate for systems and policy change. To be an effective human rights strategy, however, advocates must engage and mobilize affected individuals and communities to give voice to the indignities and rights violations that occur every day across the US and to challenge the social conditions which harm their health.
Acknowledgements
The author wishes to thank Jeffrey Sheehan and Joscelyne Kravitz for their assistance with research for this paper. I also wish to thank Joel Teitelbaum and Martha Davis for their helpful comments on early drafts.
Elizabeth Tobin Tyler, JD, MA, is Clinical Assistant Professor of Family Medicine at the Warren Alpert Medical School of Brown University and Clinical Assistant Professor of Health Services, Policy and Practice at the Brown University School of Public Health in Providence, Rhode Island, USA.
Please address correspondence to Elizabeth Tobin Tyler, the Warren Alpert Medical School of Brown University, 222 Richmond Street, Providence, Rhode Island, 02903, USA, email: Elizabeth_Tobin-Tyler@brown.edu.
References
1. J. Mann, “Health and human rights: Protecting human rights is essential for promoting health,” British Medical Journal 312 (1996), p. 924.
2. The World Health Organization Commission on Social Determinants of Health (CSDH) defined social determinants as “[t]he complex, integrated, and overlapping social structures and economic systems that are responsible for most health inequities. These social structures and economic systems include the social environment, physical environment, health services, and structural and societal factors. Social determinants of health are shaped by the distribution of money, power, and resources throughout local communities, nations, and the world.” CSDH, “Closing the gap in a generation: Health equity through action on the social determinants of health,” CSDH final report (Geneva: WHO, 2008).
3. See P. Braveman, S. Gruskin, “Policy and practice: Poverty, equity, human rights, and health,” Bulletin of the World Health Organization 8/7 (2003), pp. 539–542; P. Braveman, “Social conditions, health equity, and human rights,” Health and Human Rights: An International Journal 12/2 (2010), p. 10. Available at http://www.hhrjournal.org/2013/08/26/social-conditions-health-equity-and-human-rights.
4. US Institute of Medicine of the National Academies, U.S. health in international perspective: Shorter lives, poorer health (Washington, DC: Institute of Medicine, 2013), pp. 1–4; See also, S. Bezruchka, “American experiences,” in D. Raphael (ed), Tackling health inequalities: Lessons from international experiences (Toronto: Canadian Scholars Press, 2012), pp. 33–62.
5. C. J. Murray, J. Abraham, M. K. Ali, et al., “The state of US health, 1990–2010: Burden of diseases, injuries, and risk factors,” Journal of the American Medical Association 310/6 (2013), p. 598.
6. Ibid., p. 602.
7. See M. Marmot, “Social determinants of health inequalities,” Lancet 365 (2005), pp. 1099–1104; J. Banks, M. Marmot, Z. Oldfield, et al., “Disease and disadvantage in the United States and in England,” Journal of the American Medical Association 295/17 (2006), pp. 2037–2045.
8. P. Aka, “Analyzing U.S. commitment to socioeconomic human rights,” Akron Law Review 39 (2006), p. 423.
9. Universal Declaration of Human Rights (UDHR), G.A. Res. 217A (III) (1948), Art. 25. Available at http://www.un.org/en/documents/udhr/index.shtml.
10. See B. Meier, “Global health governance and the contentious politics of human rights: Mainstreaming the right to health for public health advancement,” Stanford Journal of International Law 46 (2010), pp. 4–5.
11. Braveman (2010, see note 3), p. 10.
12. G. MacNaughton, “The human right to health care in the United States: Health care for all,” Clearinghouse Review: Journal of Poverty Law and Policy 45/5–6 (2011), p. 210; G. Backman, P. Hunt, R. Khosla, et al., “Health systems and the right to health: An assessment of 194 countries,” Right to Health 372 (2008), p. 2048. Available at http://www.who.int/medicines/areas/human_rights/Health_System_HR_194_countries.pdf.
13. J. Ruger, Health and social justice (Oxford: Oxford University Press, 2010), p. 119.
14. See generally, Braveman (see note 3).
15. S. Gruskin, E. Mills, and D. Tarantola, “History, principles, and practice of health and human rights,” Lancet 370 (2007), p. 450. Available at http://globalhealth.usc.edu/en/Research And Services/Pages/~/media/6B72A0A151174FB1B9E7D4A836A0B000.ashx.
16. World Health Organization, A conceptual framework for action on the social determinants of health (Geneva: WHO, 2010).
17. S. Burris, “Introduction: Merging law, human rights, and social epidemiology,” Journal of Law, Medicine, and Ethics 30/4 (2002), p. 501.
18. L. Gostin, “Meeting basic survival needs of the world’s least healthy people: Toward a framework convention on global health,” Georgetown Law Journal 96 (2008), p. 382.
19. The term “American exceptionalism” has taken on multiple meanings in political and social discourse. Michael Ignatieff describes three elements of exceptionalism that are helpful to the discussion here: “First, the United States signs on to international human rights and humanitarian law conventions and treaties and then exempts itself from their provisions by explicit reservation, nonratification, or noncompliance. Second, the United States maintains double standards: judging itself and its friends by more permissive criteria than it does its enemies. Third, the United States denies jurisdiction to human rights law within its own domestic law, insisting on the self-contained authority of its own domestic rights tradition.” M. Ignatieff, American exceptionalism and human rights (Princeton, NJ: Princeton University Press, 2005), p. 3.
20. W. Henderson, “Advancing human rights and justice for all,” Clearinghouse Review: Journal of Poverty Law and Policy, 45/5–6 (2011), p. 254; H. Lewis, “‘New’ human rights? U.S. ambivalence toward the international economic and social rights framework,” in C. Soohoo, C. Albisa, M. F. Davis (eds), Bringing human rights home: A history of human rights in the United States (Westport, CT: Praeger, 2008), vol. 1, pp. 115–119.
21. P. Alston, “Putting economic, social, and cultural rights back on the agenda of the United States,” in W. Schulz (ed), The future of human rights: U.S. policy for a new era (Philadelphia: University of Pennsylvania Press, 2008), p. 129, citing remarks by Public Delegate Marc Leland, ‘‘Item 10: Economic, social and cultural rights,’’ at the 60th Session of the United Nations Commission on Human Rights, March 29, 2004.
22. See ibid., pp. 128–132.
23. Lewis (see note 20), p. 119.
24. E. Tars and D. Bhattari, “Opening the door to the human right to housing: The universal periodic review and strategic federal advocacy for a rights-based approach to housing,” Clearinghouse Review: Journal of Poverty Law and Policy 45/5–6 (2011), p. 202.
25. C. Lopez, D. Finger, M. Jain, et al., “Redefining human rights lawyering through the lens of critical theory: Lessons for pedagogy and practice,” Georgetown Journal of Poverty Law and Policy 18 (2011), p. 395.
26. Tars (see note 24), pp. 204–205.
27. A. Yamin, “The right to health under international law and its relevance to the United States,” American Journal of Public Health 95/7 (2005), p. 1157.
28. D. Orentlicher, “Rights to health care in the US: Inherently unstable,” American Journal of Law and Medicine 38/326 (2012), pp. 326–347.
29. Ibid.
30. See generally, National Federation of Independent Business v. Sebelius (2012) 132 S.Ct. 2566.
31. Congressional Budget Office, Estimates for the insurance coverage provisions of the Affordable Care Act updated for the recent Supreme Court decision (July 24, 2012).
32. MacNaugton (see note 12), p. 214.
33. The website of the Robert Wood Johnson Foundation has many such examples; see http:// www.rwjf.org.
34. S. Burris, “From health care law to the social determinants of health: A public health law research perspective,” University of Pennsylvania Law Review 159 (2011), p. 1653; See generally, L. Berkman, I. Kawachi, (eds), Social epidemiology (New York: Oxford University Press, 2000); See also, N. Krieger, Epidemiology and the people’s health: Theory and context (Oxford: Oxford University Press, 2011).
35. Braveman (2010, see note 3), p. 8.
36. Burris (see note 34).
37. Ibid.
38. See generally, R. Rector and R. Sheffield, “Understanding poverty in the United States: Surprising facts about America’s poor,” Executive summary, Backgrounder 2607 on poverty and inequality (Washington, DC: Heritage Foundation, September 13, 2011). Available at http://www.heritage.org/research/reports/2011/09/understanding-poverty-in-the-united-states-surprising-facts-about-americas-poor.
39. See generally, J. Iceland, Poverty in America: A handbook (Berkeley, CA: University of California Press, 2006).
40. Ibid., p. 70.
41. Lopez et al. (see note 25), p. 358.
42. H. Shaefer and K. Edin, “Extreme poverty in the United States, 1996 to 2011,” Policy Brief 28 (Ann Arbor, MI: National Poverty Center, February 2012), pp. 2, 4.
43. See generally, L. Siegel, K. Stewart, and N. Ferrell, Human rights in the U.S.: Opinion research with advocates, journalists, and the general public (Washington, DC: Belden Russonello and Stewart for The Opportunity Agenda, 2007). Available at http://opportunityagenda.org/files/field_file/Human%20Rights%20Report%20-%202007%20public%20opinion.pdf.
44. Ibid., p. 4.
45. Ford Foundation, Close to home: Case studies of humanitarian rights work in the United States (New York: Ford Foundation, 2004), p. 16.
46. Ibid.
47. See generally, Lopez et al. (see note 25).
48. M. Martinson, “Income inequality in health at all ages: A comparison of the United States and England,” American Journal of Public Health 102/11 (2012), pp. 2049–2056.
49. For a description of the concepts of legal empowerment and social accountability, see generally, V. Maru, “Allies unknown: Social accountability and legal empowerment,” Health and Human Rights: An International Journal, 12/1 (2010), pp. 83-93.
50. See Graham v. Florida (2010) 130 U.S. 2011, 2033-2034 (overturning the sentencing to life without parole of a subset of juvenile offenders); Roper v. Simmons (2005), 543 U.S. 551, 576–578 (rejecting the juvenile death penalty); Lawrence v. Texas (2003), 539 U.S. 558, 572–573 (overturning state criminalization of consensual homosexual acts).
51. Lopez et al. (see note 25), p. 345.
52. See ibid., p. 333.
53. See A. Redlich, “Who will litigate constitutional issues for the poor,” Hastings Constitutional Law Quarterly 19 (1992).
54. C. Soohoo and J. Goldberg, “The full realization of our rights: Right to health in state constitutions,” Case Western Reserve Law Review 60 (2010), p. 1001.
55. For a list of state court opinions that cite international human rights law, see Siegel et al. (see note 41), p. 5.
56. M. Davis, “The spirit of our times: State constitutions and international human rights,” New York University Review of Law and Social Change 30/359 (2006), pp. 4–7.
57. Soohoo, et al. (see note 54), p. 1036.
58. Ibid. p. 1033.
59. N.Y. Const. art. 17, sec. 3. Available at http://www.dos.ny.gov/info/constitution.htm.
60. N.Y. Const. art. 17, sec 1. Available at http://www.dos.ny.gov/info/constitution.htm. For an excellent discussion of the potential for using these provisions of the New York Constitution to challenge failure by the state to enforce reproductive health rights, see Davis (see note 56).
61. Soohoo, et al. (see note 54), pp. 1001–1002.
62. The website of the Vermont Workers’ Center details the principles on which this movement was built:
- Every person is entitled to comprehensive, quality healthcare.
- Systemic barriers must not prevent people from accessing necessary healthcare.
- The cost of financing the healthcare system must be shared fairly.
- The healthcare system must be transparent in design, efficient in operation and accountable to the people it serves.
- As a human right, a healthcare system that satisfies these principles is the responsibility of government to ensure.
Vermont Workers’ Center, Building a grassroots movement for the human right to healthcare. Available at http://www.workerscenter.org/hchrhistory.
63. MacNaughton (see note 12).
64. A. Rudiger, “Reviving progressive activism: how a human rights movement won the country’s first universal health care law,” New Politics Online Feature (New York: New Politics, November 6, 2011). Available at http://newpol.org/content/reviving-progressive-activism-how-human-rights-movement-won-country’s-first-universal-health.
65. Ford Foundation (see note 45), pg. 9.
66. See, for example, J. Sabonis, “Using a human rights framework at the Maryland legal aid bureau,” Clearinghouse Review: Journal of Poverty Law and Policy 44/9–10 (2011), pp. 450–458.
67. Maru (see note 49), p. 89.
68. Lopez et al. (see note 25), p. 361.
69. Sabonis (see note 66).
70. See A. Houseman, “Restrictions by funders and the ethical practice of law,” Fordham Law Review 67 (1999), pp. 218–240; R. Diller, E. Savner, A call to end federal restrictions on legal aid for the poor (New York: Brennan Center for Justice at New York University School of Law, 2009), pp. 9–10.
71. Lopez et al. (see note 25), p. 352.
72. Ford Foundation, (see note 45), p. 11.
73. Aka (see note 8), pp. 439–440.
74. Maru (see note 49), p. 88.
75. Lopez et al. (see note 25), p. 347, citing M. Davis, “The pendulum swings back: Poverty law in the old and new curriculum,” Fordham Urban Law Journal 1391 (2007), pp. 1410–1411.
76. Legal aid programs that prioritize human rights, connect individual advocacy with systemic reform, as J. Peter Sabonis describes: “Beginning with the premise that clients, because of their humanity, are entitled to civil and economic rights, we hoped to trigger both systemic and individual advocacy that was characteristic of our early history: aggressive, creative, client-centered, and movement-oriented.” Sabonis (see note 66), p. 452.
77. Maru (see note 49), p. 83.
78. C. Soohoo, C. Albisa, M. F. Davis (eds), Bringing human rights home: A history of human rights in the United States (Westport, CT: Praeger, 2008), vol. 2, p. 97.
79. Lopez et al. (see note 25), p. 350.
80. Maru (see note 49), p. 84; see also, Sabonis (see note 66), p. 454, describing how, in reframing its work as human rights work, Maryland Legal Aid Bureau used data about housing supply and demand to demonstrate a lack of government accountability.
81. Burris (see note 17), p. 499.
82. Maru (see note 49), p. 88.
83. E. Lawton, M. Sandel, S. Morton, et al., “Medical-legal partnership: A new standard of care for vulnerable populations,” in E. Tobin Tyler, E. Lawton, K. Conroy, et al. (eds), Poverty, health and law: Readings and cases for medical-legal partnership (Durham, NC: Carolina Academic Press, 2011), p. 74.
84. B. Zuckerman, E. Lawton, and S. Morton, “From principle to practice: Moving from human rights to legal rights to ensure child health,” Archives of Disease in Childhood 9/2 (2007), pp.100–101.
85. A. Beck, M. D. Klein, J. K. Klein, et al., “Identifying and treating substandard housing cluster using a medical-legal partnership,” Pediatrics 130/5 (2012), pp. 831–838.
86. Ibid., p. 834.
87. See generally, Beck et al. (see note 85).
88. Ibid., p. 835.
89. Lawton et al. (see note 83), p. 76.