Human rights in patient care: A theoretical and practical framework
Jonathan Cohen and Tamar Ezer
Health and Human Rights 15/2
Published December 2013
Abstract
The concept of “human rights in patient care” refers to the application of human rights principles to the context of patient care. It provides a principled alternative to the growing discourse of “patients’ rights” that has evolved in response to widespread and severe human rights violations in health settings. Unlike “patients’ rights,” which is rooted in a consumer framework, this concept derives from inherent human dignity and neutrally applies universal, legally recognized human rights principles, protecting both patients and providers and admitting of limitations that can be justified by human rights norms. It recognizes the interrelation between patient and provider rights, particularly in contexts where providers face simultaneous obligations to patients and the state (“dual loyalty”) and may be pressured to abet human rights violations.
The human rights lens provides a means to examine systemic issues and state responsibility. Human rights principles that apply to patient care include both the right to the highest attainable standard of health, which covers both positive and negative guarantees in respect of health, as well as civil and political rights ranging from the patient’s right to be free from torture and inhumane treatment to liberty and security of person. They also focus attention on the right of socially excluded groups to be free from discrimination in the delivery of health care. Critical rights relevant to providers include freedom of association and the enjoyment of decent work conditions. Some, but not all, of these human rights correspond to rights that have been articulated in “patients’ rights” charters.
Complementary to—but distinct from—bioethics, human rights in patient care carry legal force and can be applied through judicial action. They also provide a powerful language to articulate and mobilize around justice concerns, and to engage in advocacy through the media and political negotiation. As “patients’ rights” movements and charters grow in popularity, it is important to link patient rights back to human rights standards and processes that are grounded in international law and consensus.
Introduction
Patient care is a discrete and important aspect of the right to health that merits attention and scrutiny as a human rights issue. A vast and severe range of human rights violations occur in the patient care context that violate rights in addition to the right to health, including many civil and political rights. In response to growing concern about this abuse in many parts of the world, the phrase and concept “human rights in patient care” has recently grown in usage as a framework for monitoring, documenting, and analyzing abuses in patient care settings, and in some cases, holding governments and other parties accountable. This article outlines a framework for human rights in patient care that is closely related both to the right to health and to the more colloquial notion of “patients’ rights” but is distinct from them—as well as from complementary frameworks such as patient safety and bioethics—in important ways.
Instead of the humane and appropriate health care expected, patients and health providers in many settings encounter a variety of abuses that affront basic human dignity and jeopardize health outcomes. These abuses range from pervasive violations of patients’ rights to informed consent, confidentiality, privacy, and non-discrimination to more egregious abuses, including torture and cruel, inhuman, and degrading treatment. Health providers likewise may face abuses such as unsafe working conditions, sanctions for providing evidence-based health care, limits on their freedom of association, and denial of due process when patients make complaints against them.
The concept of human rights in patient care refers to the theoretical and practical application of general human rights principles to the patient care context, particularly to interactions between patients and providers. It applies rights principles universally to a context or setting. While centered on patients, it does not limit rights to a particular group of people. Dorland’s Medical Dictionary defines “patient care” as “the services rendered by members of the health profession and non-professionals under their supervision for the benefit of the patient.”1 This differs from “health care,” where services are provided “for the purposes of promoting, maintaining, monitoring, or restoring health.” 2 Patient care highlights patients as fundamental agents and the ultimate beneficiaries of services. The focus on patients, while not exclusive, is consistent with the way the human rights approach helps to identify and address vulnerabilities.
The human rights lens reveals issues of discrimination and social exclusion that often underlie abuse against patients. This is critical, since abuses against groups such as people living with HIV, ethnic minorities, sexual and gender minorities, people who use drugs, and people with disabilities are especially rife in health settings.3 Often these abuses are related to the perception of groups as deviant or in need of curative forms of “treatment,” leading to horrific abuses in psychiatric facilities, drug rehabilitation centers, detention centers for sex workers, and similar settings. In a recent report, the Special Rapporteur on torture recognized the particular vulnerability of marginalized groups to torture and ill treatment in health settings, citing “[s]tructural inequalities, such as the power imbalance between doctors and patients, exacerbated by stigma and discrimination.”4 The Campaign to Stop Torture in Health Care, launched in 2011 by a coalition of organizations working in the fields of health and human rights, highlighted some of the most egregious of these abuses such as forced sterilization of Roma women and women living with HIV, forced detention and punishment of people who use drugs, and unjustified denial of pain relief.5 Concretely, the human rights in patient care approach calls for a focus on the most marginalized and vulnerable in the formulation of health law and policy, guidelines and trainings for health care providers, and advocacy and litigation to address violations.
At the same time, the concept of human rights in patient care recognizes health care providers as important actors, whose rights must be respected both as a matter of principle and for the benefit of the patient. The relationship between patient and provider rights is critical. Providers are unable to provide high-quality care unless their rights are respected and they can work under decent conditions with professional independence. There is no shortage of examples of health providers who have been punished for providing evidence-based health care to their patients, ordered to destroy medical records or disclose confidential health information to the state, or coerced into participating in (or covering up) torture and crimes against humanity. Even in open societies, health providers may be denied safe working conditions, punished for alleged ethical breaches without any due process, or forced to provide a standard of care that violates their ethical principles.6 These violations not only offend basic human dignity, but also pose a risk to patients. These violations thrive on a culture of disrespect and abuse that has the potential to harm everyone who comes into contact with the health care system. In this way, the human rights in patient care approach does not pit patients against providers, but rather recognizes links that may lead to joint advocacy to address systemic issues.
A related concept to human rights in patient care is “dual loyalty,” or a health provider’s “simultaneous obligations, express or implied, to a patient and to a third party, often the state.”7 Such simultaneous obligations can, depending on the circumstances, pose a risk of human rights violations. In cases where the interests of the patient and the state are aligned, dual loyalty poses little risk. However, where they conflict, the result is often that doctors are compelled to abuse the rights of their patients. The International Dual Loyalty Working Group, convened by Physicians for Human Rights in 1993, observed that, in both repressive and open societies, “Governments and other third parties often demand that health professionals put allegiance to their patients aside, in deference to the demands of these powerful actors—often in a manner that violates patients’ human rights.” The Working Group provides examples of contexts that may give rise to dual loyalty conflicts, including health practice under repressive governments; closed institutions such as prisons and the military; and open societies with institutionalized bias against women, ethnic and religious minorities, immigrants and refugees, and socially stigmatized patients.8
The Working Group goes on to describe six common types of human rights violations that stem from dual loyalty conflicts. Many of these violations will seem familiar to those who advocate for the health and human rights of marginalized populations:
- Using medical skills or expertise on behalf of the state to inflict pain or physical or psychological harm that is not a legitimate part of medical treatment;
- Subordinating independent judgment, whether in therapeutic or evaluative settings, to support conclusions favoring the state or other third party;
- Limiting or denying medical treatment or information related to treatment of an individual to effectuate the policy or practice of the state or other third party;
- Disclosing confidential patient information to state authorities or other third parties in circumstances that violate human rights;
- Performing evaluations for state or private purposes in a manner that facilitates violations of human rights;
- Remaining silent in the face of human rights abuses committed against individuals and groups in the care of health professionals.9
Dual loyalty sheds light on the causes and manifestations of human rights abuses in patient care, and it also provides a framework for preventing abuse by resolving dual loyalty conflicts in a fair and transparent manner.
The International Dual Loyalty Working Group has produced guidelines to assist health providers in resolving dual loyalty conflicts, which can be incorporated into medical education, training, and policy as part of a broader global campaign to promote human rights in patient care.
The concept of human rights in patient care thus widens out from the individual patient-provider relationship to examine systemic factors and state responsibility in the provision of patient care. As Health and Human Rights: A Reader explains, “a human rights perspective, which takes individual rights to information, privacy, and bodily integrity seriously and treats all people as equals” transforms “government approaches to the physician-patient relationship.”10 Additionally, the human rights in patient care concept refers not just to entitlements for actual patients, but also to human rights standards in the provision of care that concern health providers and the entire community. It calls for a pervasive human rights frame to govern the delivery of care to patients in all its aspects, which also highlights equality, participation, transparency, and accountability concerns.
Discussion
Applicable human rights law
As noted above, human rights principles require that services to patients meet standards set out in international and regional human rights norms and agreements. These standards can be found in major treaties such as the International Covenant on Civil and Political Rights (ICCPR), International Covenant on Economic, Social, and Cultural Rights (ICESCR), Convention Against Torture (CAT), African Charter on Human and Peoples’ Rights (ACHPR), European Convention on the Protection of Human Rights and Fundamental Freedoms (ECHR), European Social Charter (ESC), and various thematic covenants related to women (Convention on the Elimination of All Forms of Discrimination against Women: CEDAW), children (Convention on the Rights of the Child: CRC), people with disabilities (Convention on the Rights of Persons with Disabilities: CRPD), racial minorities (International Convention on the Elimination of All Forms of Racial Discrimination: ICERD), and other populations.11 The provisions of these treaties have been interpreted by human rights bodies to prohibit numerous forms of abuse in health settings. For example, the right to liberty and security of the person has been held to prohibit institutionalization without due process of people with mental illness; the right to privacy has been held to prohibit unauthorized disclosure of personal health data; the rights to bodily integrity and security of the person have been held to prohibit the administration of medicine to a child against parents’ wishes; and the right to freedom from cruel, inhuman, or degrading treatment or punishment has been held to oblige governments to secure the adequate health and well-being of prisoners.12 There is ample room to expand this jurisprudence by bringing new cases of abuse and arguing for expansive interpretations of human rights treaties to apply to diverse health care delivery contexts.
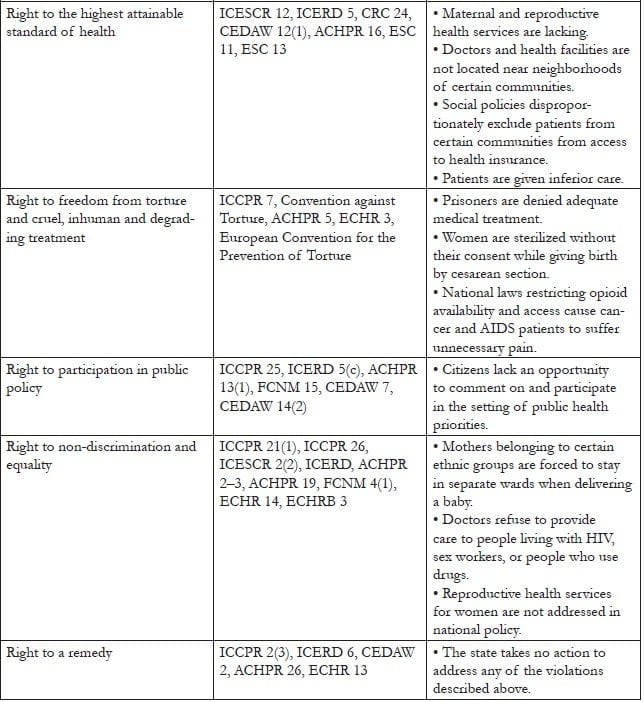
Table 1 lists internationally and regionally recognized rights relevant to patients, along with applicable treaty provisions and examples of violations. It is important to note that the finding of a human rights violation depends on the circumstances and is a matter of interpretation based on the facts of the case. In any particular case, rights may be judged to have been violated or not. Human rights law is an evolving field, and many human rights violations are not directly addressed by existing legal precedents. Through ongoing documentation, advocacy, and litigation, advocates can build a stronger body of jurisprudence protecting human rights in patient care.
Table 1. Human rights of patients
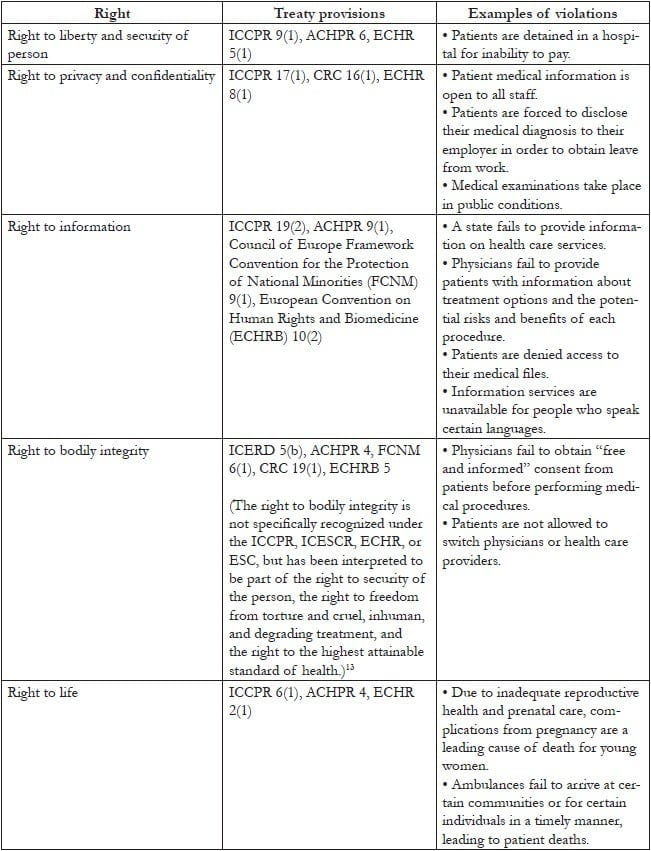
A particularly important (though not exclusive) source of international human rights law relevant to patient care is the right to the highest attainable standard of health found in Article 12 of the ICESCR. The human rights framework highlights government responsibility to respect human rights itself, protect against violations by third parties, and fulfill the conditions necessary for the realization of rights. While the right to health is sometimes understood to focus only on positive guarantees for the progressive realization of the availability, accessibility, acceptability, and quality of health care for all, it also incorporates negative guarantees for the assurance of freedom from abuse and discrimination by the state and third parties within health care service delivery. The Committee on Economic, Social and Cultural Rights, the expert committee responsible for interpreting the ICESCR, makes numerous references to such abuses in its General Comment No. 14: The Right to the Highest Attainable Standard of Health. Among the Committee’s relevant observations are the following:
- The rights to human dignity, prohibition against torture, privacy, and access to information address integral components of the right to health; (paragraph 3)
- The right to health contains freedoms such as “the right to control one’s health and body, including sexual and reproductive freedom, and the right to be free from interference, such as the right to be free from torture, non-consensual medical treatment and experimentation.” (paragraphs 4, 8)
- The right of accessibility of health care “includes the right to seek, receive and impart information and ideas concerning health issues. However, accessibility of information should not impair the right to have personal health data treated with confidentiality.” (paragraph 12(b))
- The right of acceptability of health care provides that “all health facilities, goods and services must be respectful of medical ethics … as well as being designed to respect confidentiality,” and also refers to “the right to have personal health data treated with confidentiality.” (paragraph 12)
- The obligation to protect the right to health includes the duty of States “to ensure that medical practitioners and other health professionals meet appropriate … ethical codes of conduct.” (paragraph 35)
- The right of accessibility includes the right to access health care without discrimination, “especially to the most vulnerable and marginalized sections of the population.” This requires particular attention to the needs of ethnic minorities, persons with disabilities, and persons with HIV/AIDS. (paragraph 12)14
An important distinction between human rights in patient care and the right to health, therefore, is that the former encompasses additional rights that pertain to the delivery of services to patients. By the same token, the latter also encompasses the vast range of human rights that fall outside the health care delivery context, but nevertheless play an important role in determining health outcomes. Often referred to as “underlying determinants of health,”these may include not only social and economic rights to adequate housing, potable water and food, but also civil and political rights such as freedom from violence, censorship, discrimination, and torture—all of which can have serious health consequences.15 Human rights in patient care, by contrast, specifically address stakeholder rights inside health care settings—be they hospitals, clinics, outreach facilities, places of detention, or private homes—and in the particular context of patient care, which may be defined as services rendered by health providers for the benefit of patients. It may thus be said that human rights in patient care and the right to health contain overlapping subsets—the former encompasses a series of general rights that include the right to health, and the latter encompasses a series of health contexts that include the context of patient care.
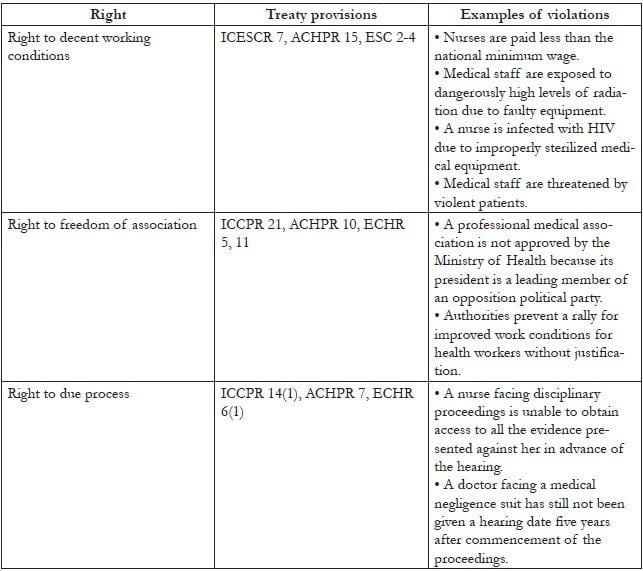
Moreover, human rights apply not only to patients, but to providers as well. Table 2 provides a listing of three key clusters of rights relevant to providers, along with applicable treaty provisions and examples of violations.
Table 2. Human rights of providers
In addition to the right to health discussed above, it is important to differentiate human rights in patient care from other paradigms commonly applied to health care settings. These frameworks include patients’ rights, patient safety, and bioethics. The following sections situate human rights in patient care in this landscape.
Human rights and patients’ rights
The modern movement for patients’ rights emerged out of increasing concern about human rights abuses in health care settings, particularly in countries where patients are assuming a greater share of health care costs and thus expect to have their rights as “consumers” respected in return.16 In the last 50 years, specific patients’ rights have been codified in key regional instruments. In the European context, this includes the European Convention on Human Rights and Biomedicine (ECHRB), the World Health Organization’s Declaration on the Promotion of Patients’ Rights in Europe, and the European Charter of Patients’ Rights. In other parts of the world, national patient charters echo this development.17
To a certain extent, the codification of patients’ rights can play a role in educating people about rights and advancing the struggle to establish human rights in patient care. For instance, in South Africa, Professors London and Balwin-Ragaven note, “One of the key mechanisms developed by the Department of Health to operationalize human rights has been the Patients’ Rights Charter,” which has set “a common standard for achieving the range of health rights.”18 The foundational Health and Human Rights: A Reader suggests the development of “an international patient bill of rights” to bring “universal recognition of the rights of patients.”19
Partners of the Open Society Foundations (OSF) in Eastern Europe and Central Asia have found the clear, wide-ranging formulation of patients’ rights in the European Charter of Patients’ Rights to be a useful frame for assessing gaps in national legal frameworks and in rights trainings for patients and providers.20 The Charter systemizes patient rights into 14 concrete provisions (see Table 3). Developed in 2002 by the Active Citizenship Network (ACN), the Charter emerged from a grassroots movement across Europe calling for patients to play a more active role in shaping the delivery of health services and attempting to translate right-to-health documents into meaningful provisions. ACN identified health care as a critical arena for civic engagement and aimed to change patients from “mere targets and users of health services to active citizens engaged in producing information and participating in policymaking.”21 Nonetheless, the Charter is not a human rights document, and it is important to note that the pharmaceutical company Merck & Co. helped fund this movement, which brings with it financial interests in tension with human rights.22
Although the Charter is not legally binding, it has had an impact on law and policy. Patients’ rights groups across Europe, particularly in countries such as Bulgaria with an eye towards European Union accession, have successfully lobbied their national governments for adoption of the rights in the Charter, and it has been used as a reference point to monitor and evaluate health care systems across Europe.23 In September 2007, the European Economic and Social Committee approved an initiative opinion on patients’ rights, where it explicitly welcomed the European Charter of Patients’ Rights.24
However, the patients’ rights approach has fundamental limitations and differs from that of human rights in patient care in important ways. First, patients’ rights link to a consumer framework. Consumer rights are different from human rights. Consumer rights do not inhere in patients because they are human, but rather because they are recipients of a transaction. In this way, consumer rights stem from principles of neoliberal economic theory and more closely resemble contractual rights. They do not have the “inherent,” “inalienable,” or “universal” qualities of human rights.25
Second, patients’ rights leave out the rights of other stakeholders in health care delivery, focusing exclusively on patients. In contrast, human rights apply to everyone, and their universality is central to their power. Recognizing that health care providers enjoy the same human rights as everyone else (rather than positing special rights for patients as against those who provide them with health care) is more consistent with universal human rights principles and essential to nurturing a culture of respect for human rights within health care delivery systems.
Moreover, the patients’ rights paradigm does not automatically recognize the need to place limitations on rights in the health context—whether because of compelling policy objectives that can be shown to be rational and proportionate to rights violations in a free and democratic society, or because of the need to balance competing patient claims for health care services with the public good in a world of limited resources. The human rights framework enables a more systemic, balanced approach that recognizes that the rights of no single patient are absolute. Limitations on rights are made to conform to a human rights assessment of factors such as their appropriateness, likely effectiveness, proportionality to the abuse involved, and the presence of alternatives.26 Courts go through this analysis in placing limitations on human rights in the health care context, often in response to express or implied limitation clauses in national constitutions.27
Finally, patients’ rights are meaningless and subject to manipulation if they are not rooted in general human rights principles. For example, the European Charter of Patients’ Rights recognizes the rights of patients to “innovation” and “free choice,” neither of which is a recognized right of general application. The right to innovation can be based in the general right to enjoy the benefits of scientific progress.28 However, without this link, it is an “invented” right that could be used to, for example, justify a system of monopoly patents on pharmaceuticals in exchange for investment in research and development of innovative drugs. Similarly, the right to free choice should be grounded in the right to liberty and security of person and has important implications in areas such as the right to choose a physician based on adequate information.29 Without this link, it could be used to justify controversial direct-to-consumer advertising of pharmaceutical products. (The full statement of this right is: “Each individual has the right to freely choose from among different treatment procedures and providers, on the basis of adequate information.”) Even the basic right of access under the Charter benefits from the lens of human rights and its focus on non-discrimination and equality.
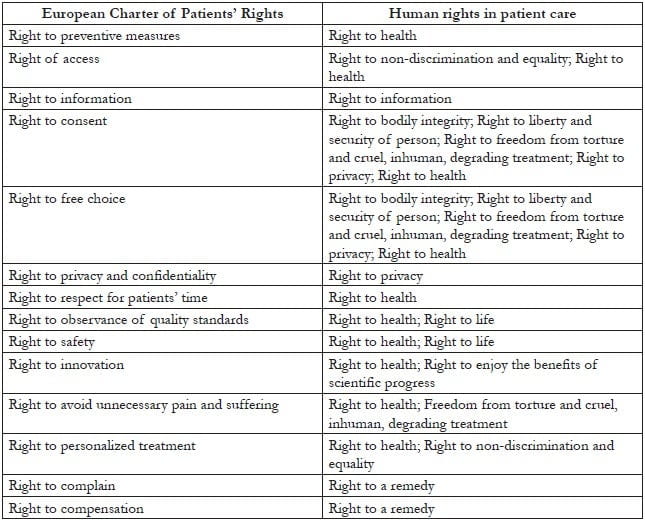
It is thus critical, where possible, to link patient rights back to human rights standards grounded in international law and consensus—which, as noted above, allow for rights to be limited in some circumstances. Table 3 cross-references the rights in the European Charter of Patients’ Rights with human rights of general application from which they may be derived. This cross-referencing allows for complementary use of patients’ rights codes, which may provide helpful specificity and context. Many patient charters also delineate providers’ corresponding responsibilities to patients’ rights, which could be useful in developing provider guidelines and trainings.30 At the same time, it is important that such cross-referencing—and the similarities of language between patients’ rights and corresponding human rights—not conceal the differences in the philosophical underpinnings of the two. Our aim is not to elide these differences but, on the contrary, to expose them and urge an approach that is rooted in international law and consensus, while respecting that many have found the patients’ rights framework useful. Further inquiry into the consumerist underpinnings of particular patients’ rights (for example, “the right to innovation”) as against the legal underpinnings of roughly corresponding human rights (for example, “the right to the benefits of scientific progress”) would be an important step in developing and justifying human rights in patient care as a unique and value-adding concept.
Table 3. Cross-referencing patients’ rights with human rights in patient care
A contrast to patient safety
It is additionally important to distinguish human rights in patient care from the concept of patient safety or the promotion of quality medical care. While patients may be said to have a right to quality care and to freedom from injury, not all low-quality care rises to the level of a human rights violation for which the state is responsible. Instances of simple negligence are best characterized as a tort against individual health care providers. To constitute a human rights violation, mistreatment by a health care provider must be systemic. The state should be taking steps to address the problem systemically, such as amending policies or regulations, ensuring appropriate training, monitoring services, establishing opportunities for complaint and redress, and taking disciplinary measures where warranted. Conversely, human rights do not end with quality care. A patient may be provided with top-notch medical care without his or her consent. Indeed, human rights in patient care aims to move away from a biomedical model focusing only on the nature and quality of patient services towards one in which patients are active agents in their health care and in which their basic dignity and freedom must be respected, protected, and fostered.
A complementary framework to bioethics
The concept of human rights in patient care provides a complementary framework to bioethics with the former’s systemic approach, operational norms and procedures, and focus on advocacy. While the field and practice of bioethics applies philosophical principles such as autonomy, beneficence, justice, and non-maleficence to the patient care context (as well as to other contexts such as medical research and public health), the human rights framework applies a complementary set of legal norms (for example, freedom, security of the person, non-discrimination) that have been developed through judicial interpretation. This legal analysis enables a more systemic approach, widening from of an individual patient-provider relationship and focusing attention on the state.
Furthermore, human rights add to bioethics both “a method for arriving at concrete decisions” about how to judge complex and ethically challenging clinical interactions and a set of procedures for enforcing those decisions.31 According to the International Dual Loyalty Working Group, “[T]he four principles [of bioethics] do not provide a method for arriving at concrete decisions—particularly decisions about how to prioritize competing principles.”32 Rooted in a legal framework, in addition to operational norms, human rights brings with it procedures, such as courts and human rights commissions, to identify, adjudicate, and remedy abuses.
Significantly, the human rights framework brings a focus on advocacy. This advocacy takes place, not just through the courts, but also through the media and political negotiation. Identifying a human rights issue provides not only the possibility of a legal remedy, but also the mobilizing power of the language of rights and the shaming power of naming a rights “violator.” Human rights are much more than the legal framework to which they are linked. They provide a language to articulate and mobilize around justice concerns. Community mobilization complements litigation and often plays a critical role in advancing rights protections. Examples of this include mobilization around the recent maternal mortality case in Uganda or the forced sterilization of women living with HIV case in Namibia.33 Human rights thereby complement public health ethics, a relative of medical ethics concerned with “ensuring that public health interventions provide benefit and minimize harms, respect individuals’ dignity and rights to the greatest extent possible, and are implemented fairly.”34 While public health ethics focuses on creating professional codes to “self-regulate” and “instill trust in the profession on the part of the public,” the work of human rights “explicitly targets governments or the policies they endorse.”35 Bioethics looks internally to improve care, while human rights can take a more external, hard-hitting approach.
Conclusion
The concept of human rights in patient care provides a framework for addressing abuses in health settings and holding governments accountable for them. It has the following distinct features:
- Refers to the theoretical and practical application of general human rights principles to the context of patient care, including both patients and providers;
- Places patients at the center and focuses attention on discrimination and social exclusion;
- Recognizes the interrelation between patient and provider rights and draws on concepts of dual loyalty, which attributes much human rights abuse in health settings to health providers’ simultaneous and often conflicting obligations to their patients and the state;
- Zooms out from the individual patient-provider relationship to examine systemic issues and state responsibility;
- Includes key patient rights to liberty and security of the person; privacy; information; bodily integrity; life; highest attainable standard of health; freedom from torture, cruel, inhuman, and degrading treatment; participation in public policy; non-discrimination and equality;
- Also includes key provider rights to decent work conditions; freedom of association; and due process;
- Derives from universal and inherent human dignity, rather than the rights of patients as participants in a consumer transaction;
- Recognizes the need to place limitations on rights in the health care context, whether because of compelling policy objectives or competing resources;
- Draws on accepted international norms and jurisprudence to avoid linguistic or conceptual manipulation;
- Complements bioethics by providing a set of legally recognized and globally accepted norms and procedures for identifying systemic issues and enabling redress and mobilization.
The application of the human rights framework to patient care calls for a range of measures, such as strengthened laws, policies, and guidelines to protect the human rights of patients and providers; careful documentation of abuses within health care service delivery and legal remedies to address them; and training for patients and providers on the concept and application of human rights to patient services. In particular, it is critical to integrate human rights training for health care providers at all levels.
The other articles in this issue reflect on education, litigation, and law reform initiatives that have sought to realize the human rights in patient care framework. Along with other sets of normative standards governing patient care, human rights can contribute to health systems serving as places of treatment, care, and support for everyone.
Jonathan Cohen, B.A., JD, MPhil, is the Deputy Director of the Public Health Program at the Open Society Foundations.
Tamar Ezer, BA, JD, LLM, is the Senior Program Officer at the Law and Health Initiative of the Public Health Program at the Open Society Foundations.
Please address correspondence to Jonathan Cohen, 224 West 57th Street, New York, NY 10019, USA, email: jonathan.cohen@opensocietyfoundations.org.
References
1. Dorland’s illustrated medical dictionary, 28th ed. (Philadelphia, PA: Elsevier Health Sciences, 1994), s. v. “patient care” (emphasis added).
2. Ibid., s. v. “health care.”
3. See, for example, Aman Plus, Observance of the rights of injecting drug users in the public health system (Bishkek, Kyrgystan: Aman Plus, 2008). Available at http://www.opensocietyfoundations.org/sites/default/files/aman_20081120.pdf; Central and Eastern European Harm Reduction Network (CEEHRN), Sex work, HIV/AIDS, and human rights in Central and Eastern Europe and Central Asia (Vilnius, Lithuania: CEEHRN, 2005). Available at http://www.opensocietyfoundations.org/sites/default/files/sex%2520work%2520in%2520ceeca_report_2005.pdf; Mental Disability Rights International, Torment not treatment: Serbia’s segregation and abuse of children and adults with disabilities (Washington, DC: Mental Disability Rights International, 2007). Available at http://www.disabilityrightsintl.org/wordpress/wp-content/uploads/Serbia-rep-english.pdf; Open Society Foundations, Access to Health Care for LGBT People in Kyrgyzstan (New York: Open Society Foundations, 2007). Available at http://www.opensocietyfoundations.org/reports/access-health-care-lgbt-people-kyrgyzstan; Open Society Foundations, Roma health rights in Macedonia, Romania, and Serbia: A baseline for legal advocacy (New York: Open Society Foundations, 2013). Available at http://www.opensocietyfoundations.org/reports/roma-health-rights-macedonia-romania-and-serbia-baseline-legal-advocacy.
4. Juan Méndez, UN Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment, UN Doc. A/HRC/22/53 (2013), para. xxvi–xxix.
5. For information about the 2011 campaign, see F. Girard, “Stop torture in health care,” (New York: Open Society Foundations, March 29, 2011). Available at www.opensocietyfoundations.org/voices/stop-torture-health-care-0; For background on the forced sterilization of Roma women, see United Nations Committee on the Elimination of All Forms of Discrimination against Women, A.S. v. Hungary, UN Doc. No. CEDAW/C/36/D/4/2004 (2006). Available at http://www.escr-net.org/docs/i/1053033; For more on abuses against women living with HIV, see F. Kasiva, Robbed of choice: Forced and coerced sterilization experiences of women living with HIV in Kenya (Nairobi: African Gender and Media Initiative, 2012). Available at http://kelinkenya.org/wp-content/uploads/2010/10/Report-on-Robbed-Of-Choice-Forced-and-Coerced-Sterilization-Experiences-of-Women-Living-with-HIV-in-Kenya.pdf; and International Community of Women Living with HIV/AIDS, The forced and coerced sterilization of HIV positive women in Namibia (London: International Community of Women Living with HIV/AIDS, 2009). Available at http://www.icw.org/files/The%20forced%20and%20coerced%20sterilization%20of%20HIV%20positive%20women%20in%20Namibia%2009.pdf; For more on forced detention and punishment of people who use drugs, see Open Society Foundations, Human rights abuses in the name of drug treatment: Reports from the field (2010). Available at http://www.opensocietyfoundations.org/publications/human-rights-abuses-name-drug-treatment-reports-field; For more on unjustified denial of pain relief, see Human Rights Watch, Global state of pain treatment: Access to medicines and palliative care (June 2011). Available at http://www.hrw.org/reports/2011/06/02/global-state-pain-treatment-0.
6. International Working Group, Dual loyalty and human rights in health professional practice: Proposed guidelines and institutional mechanisms (Boston: Physicians for Human Rights, 2002), p. 12; F. Hashemian, S. Crosby, V. Iacopino, et al., Broken laws, broken lives: Medical evidence of torture by US personnel and its impact (Boston: Physicians for Human Rights, 2008). See also, L. Beletsky, T. Ezer, J. Overall, et al., Advancing human rights in patient care: The law in seven transitional countries (New York: Open Society Foundations, 2013), pp. 67–72.
7. International Dual Loyalty Working Group (see note 6), p. 11.
8. Ibid., p. 12 (emphasis added).
9. Ibid., p. 27.
10. J. Mann, S. Gruskin, M. Grodin, and G. Annas (eds), Health and human rights: A reader (New York: Routledge, 1999), p. 281.
11. Open Society Institute and Equitas, “Appendix – Thirteen health and human rights documents,” in Health and human rights: A resource guide (New York: Open Society Institute, 2007). Available at http://www.equalpartners.info/Appendix/App_TOC.html.
12. Details and citations of these holdings can be found in the following: Beletsky et al. (see note 6), pp. 19–33; and Mann et al. (see note 10). Available at http://www.equalpartners.info/Chapter1/ch1_3Which.html.
14. UN Committee on Economic, Social and Cultural Rights (CESCR), General Comment No. 14. Substantive Issues Arising in the Implementation of the International Covenant on Economic, Social and Cultural Rights, UN Doc. E/C.12/2000/4 (2000).
15. See, for example, World Health Organization, “The determinants of health” (Accessed July 31, 2012). Available at http://www.who.int/hia/evidence/doh/en/.
16. J. Fridli, New challenges in the domain of health care decisions (Budapest: Open Society Institute, 2006), p 11. Available at http://pdc.ceu.hu/archive/00003127/.
17. See, for example, Argentina Ministry of Health legislation. Available at http://leg.msal.gov.ar/bioetica.htm; The Law on the Rights of Patient, Republic of Georgia (2000). Available at http://www.healthrights.ge/legislation/national/?lang=en; Israeli Patient’s Rights Act, State of Israel (1996). Available at http://waml.haifa.ac.il/index/reference/legislation/israel/israel1.htm; Law on the Protection of Patients’ Rights, Official Gazette of the Republic of Macedonia, No. 82/08 (2008); Patients’ Charter, Uganda Ministry of Health (2009). Available at http://www.health.go.ug/Patient.pdf.
18. L. London and L. Baldwin-Ragaven, “Human rights and health: Challenges for training nurses in South Africa, Curationis 31/1 (2008), p. 7.
19. Mann et al. (see note 10), p. 281.
20. Active Citizenship Network, European charter of patients’ rights (2002). Available at http://www.patienttalk.info/european_charter.pdf.
21. Health and Social Campaigners’ Network, Patients’ rights in Europe: A citizens’ report; commissioned by Oxford Vision 2020 (summary of meeting organized by Active Citizenship Network, The European Parliament, Brussels, Feb. 28 – March 1, 2005). Available at http://archive.oxha.org/knowledge/publications/oxha_dialogue_patient_rights.pdf.
22. Ibid.
23. See Active Citizenship Network, “Monitoring patients’ rights in Europe” (Accessed October 15, 2013). Available at http://www.activecitizenship.net/patients-rights/projects/30-monitoring-patients-rights-in-europe.html.
24. Opinion of the European Economic and Social Committee on “Patients’ rights,” Official Journal of the European Union C 10/18 (2008), p. 67. Available at http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:C:2008:010:0067:0071:EN:PDF.
25. Universal Declaration of Human Rights (UDHR), G.A. Res. 217A (III) (1948), Preamble. Available at http://www.un.org/Overview/rights.html.
26. See, for example, UN Economic and Social Council, Siracusa Principles on the Limitation and Derogation Provisions in the International Covenant on Civil and Political Rights, UN Doc. E/CN.4/1985/4, Annex (1985).
27. See, for example, Soobramoney v. Minister of Health (Kwazulu-Natal) (CCT32/97) [1997] ZACC 17; 1998 (1) SA 765 (CC); 1997 (12) BCLR 1696 (27 November 1997).
28. ICESCR (see note 13), Art. 15.
29. ICCPR (see note 13), Art. 9(1).
30. See, for example, Israeli Patient’s Rights Act, Macedonian Law on the Protection of Patients’ Rights, and Ugandan Patients’ Charter (see note 17).
31. S. Marks, “The new partnership of health and human rights,” (New York: Carnegie Council for Ethics in International Affairs, May 16, 2001). Available at http://www.carnegiecouncil.org/publications/archive/dialogue/2_06/articles/650.html.
32. International Dual Loyalty Working Group (see note 6), p. 16.
33. See the campaign website, available at http://endforcedsterilisation.wordpress.com/.
34. J. Cohen, N. Kass, and C. Beyrer, “Human rights and public health ethics: Responding to the global HIV/AIDS pandemic,” in C. Beyrer and H. Pizer (eds.), Public health and human rights: Evidence-based approaches (Baltimore, MD: Johns Hopkins University Press, 2007), p. 368.
35. Ibid., p. 368; Ibid., p. 386.