The right to health in the courts of Brazil: Worsening health inequities?
Octavio Luiz Motta Ferraz
Health and Human Rights 11/2
Published December 2009
Le plus grand mal est déjà fait, quand on a des pauvres à défendre et des riches à contenir. C’est sur la médiocrité seule que s’exerce toute la force des lois; elles sont également impuissantes contre les trésors du riche et contre la misère du pauvre; le premier les élude, le second leur échappe; l’un brise la toile, et l’autre passe au travers.
— Jean-Jacques Rousseau1
Courts are, at the end of the day, never an instrument of total societal revolution . . . never a substitute for direct political action.
— Upendra Baxi2
Abstract
This article analyzes the recent and growing phenomenon of right-to-health litigation in Brazil from the perspective of health equity. It argues that the prevailing model of litigation is likely worsening the country’s already pronounced health inequities. The model is characterized by a prevalence of individualized claims demanding curative medical treatment (most often drugs) and by a high success rate for the litigant. Both elements are largely a consequence of the way Brazilian judges have interpreted the scope of the right to health recognized in Article 6 and Article 196 of the Brazilian constitution, that is, as an entitlement of individuals to the satisfaction of all their health needs with the most advanced treatment available, irrespective of its costs. Given that resources are always scarce in relation to the health needs of the population as a whole, this interpretation can only be sustained at the expense of universality, that is, so long as only a part of the population is granted this unlimited right at any given time. The individuals and (less often) groups who manage to access the judiciary and realize this right are therefore privileged over the rest of the population. This is potentially detrimental to health equity because the criterion for privileging litigants over the rest of the population is not based on any conception of need or justice but purely on their ability to access the judiciary, something that only a minority of citizens possess. This paper examines studies that are beginning to confirm that a majority of right-to-health litigants come from social groups that are already considerably advantaged in terms of all socioeconomic indicators, including health conditions. It is a plausible assumption that the model of right-to-health litigation currently prevalent in Brazil is likely worsening health inequities.
Introduction
The recognition of health as a fundamental right of everyone and a corresponding duty of the state in Article 6 and Article 196 of the 1988 Brazilian federal constitution was a momentous victory of the “sanitary movement,” a group of health professionals and experts from academia and research institutes who from the mid-1970s had been fighting for universalized access to health services and actions, for decentralization of their provision and administration, and for a change in health policy focus from curative treatment to preventative measures.3 Enactment of legal (even if constitutional) provisions does not, however, guarantee social change, let alone rapid change. This effort in Brazil to transform a system which has historically excluded the vast majority of the population into a truly universal one has proven to be (unsurprisingly) a protracted and complex task, fraught with political, financial, geographical, and cultural difficulties.4 Twenty years after redemocratization and the promulgation of the socially progressive 1988 constitution, there are still huge inequalities among individuals in the Brazilian population in all socioeconomic indicators, including health.5 It is still accurate to speak, therefore, of two Brazils (“dois Brasis”), as the French geographer Jacques Lambert proposed in 1959, so disparate as to resemble two different countries, one developed the other underdeveloped.6 In this context, which Kurt Weyland aptly named “democracy without equity,” it is not surprising that the judicial branch of the state is regarded by academics and activists as a potential forum to counter the lack of political will that hinders the full implementation of the constitutional transformative promises.7 It is necessary to inquire, therefore, if and how litigation can help in the achievement of these goals. But one must be aware that the opposite is also possible, that is, that courts may be able to achieve little to no change or, worse, might further hinder the transformative enterprise.
I suggest in this paper that the Brazilian experience should give us reason to be extremely cautious (if not skeptical) about the potential of the judiciary as a vehicle for social change in the health arena. Whereas Brazil has been experiencing what could be called an explosion of litigation, the courts might be worsening the country’s already pronounced health inequities. I suggest that this is an almost inevitable corollary of the particular model of health litigation and adjudication in Brazil. The “Brazilian model,” as I refer to it in this paper, is characterized by a prevalence of individualized claims demanding curative medical treatment (most often drugs) and by an extremely high success rate for the litigant. This model has been shaped and encouraged largely by the interpretation of the constitutional right to health that was established in the late 1990s at the highest level of the Brazilian judiciary system, the Supreme Federal Tribunal (the “Supremo Tribunal Federal” or STF), and later became dominant in the rest of the Brazilian judiciary. In this interpretation, the right to health is an individual entitlement to the satisfaction of one’s health needs with the most advanced treatment available, irrespective of costs.
I argue that this interpretation of the right to health — which excludes nothing from its scope — and the model of litigation that it encourages are inadequate and potentially detrimental to health equity for two reasons. First, given that resources are always limited in relation to the health needs of the population, it is simply impossible to provide everyone with the most advanced treatment for their health needs. An interpretation of the right to health that ignores resource limitations can only be sustained at the expense of universality, that is, so long as only a small part of the population is granted the unlimited right to any benefits at any given time. The minority of individuals and (less often) groups who are granted this unlimited right via the judiciary are therefore privileged over the rest of the population. Second, access to courts is random at best and, more frequently, skewed toward those people whose health conditions are already comparatively better due to their better economic conditions and hence better access to the other so-called “social determinants” of health (such as education, housing, and nutrition). Under these circumstances, which the empirical studies examined in this article confirm, it is plausible that Brazil’s current model of right-to-health litigation does not improve health equity. In fact, the litigation may exacerbate health inequities.
Whether this model can be changed or is too deeply ingrained in the Brazilian legal culture is an important and complex issue, but one beyond the scope of this article, as is any substantial discussion of what consequences the conclusions offered below might have on the question of how legitimate it is for courts to interfere with social and economic policies.8 My focus here is to draw attention to the likely perverse effects of the current Brazilian model, effects that should, I suggest, be taken very seriously by those who support the courts as being potential enforcers of the right to health.
In what follows, I first describe what I call the Brazilian model of right-to-health litigation. The article then offers a conception of health equity that might be usefully applied to test the Brazilian model. This framework is then used to analyze the impact of the Brazilian model on health equity, making use of the data that is now emerging from empirical studies on right-to-health litigation. Finally, the article concludes by arguing that the Brazilian model is not improving health equity and may actually be worsening the already pronounced health inequities of the country.
The Brazilian model of right-to-health litigation
The phrase “right-to-health litigation” can be interpreted in several different ways, depending on how one interprets the scope of the right to health itself. Here, I restrict this phrase to mean litigation in which the claimant demands the provision of some health benefit or treatment from the state based on the constitutional right to health. Such focus seems justified for several reasons. First, it is this type of right-to-health claim that provokes controversy about the appropriate role of courts in the adjudication of matters involving social and economic policy. Second, it was the rise and significant growth of this type of claim that created the current problem in the Brazilian context, the so-called “epidemics of litigation,” discussed further below. Finally, this type of claim has the largest potential impact on health equity due to the inevitable interference of court orders with the state’s health policies.
The defining features of this “Brazilian model” are related to the profile of claims (the litigator and the object of litigation) and the outcome of litigation (the rates of success and failure of litigation). As to the profile of claims, the vast majority of right-to-health cases in Brazil to date have been filed by individual claimants and have concerned the provision of curative medical treatment (mostly medicines) which can be enjoyed individually. As to the outcome of litigation, the Brazilian model is characterized by an extremely high success rate for claimants. This model, I suggest, is encouraged by the dominant interpretation of the right to health by the Brazilian judiciary. As noted above, most Brazilian judges and courts, including the STF, see the right to health as an individual entitlement to the satisfaction of all one’s health needs with the most advanced treatment available, irrespective of costs.9
The establishment of this Brazilian model is strongly related to the successful campaign of persons with HIV/AIDS, begun in the 1980s, to receive free treatment from the state. A high point of this fight was the 1996 enactment by the Brazilian Parliament (the “National Congress”) of Law 9.313/96, which imposes a duty on the state to provide free medication to all patients infected with HIV or suffering from AIDS.10 When it became clear that the speed of innovation in HIV/AIDS diagnosis and treatment was not matched by the integration of new technologies in the state’s health program, HIV/AIDS sufferers turned to the courts to try to bridge that gap.
Their judicial strategy proved highly successful.11 In 1996, the first claimants received favorable interim decisions from first instance judges in São Paulo, Rio de Janeiro, and Florianopolis. These decisions were confirmed in appeals all the way up the judiciary’s hierarchy, reaching the STF in the late 1990s, when, in a landmark decision that was to become a kind of de facto binding precedent, the STF provided the rationale upon which most of the subsequent successful cases have been based.12 The relevant passage of this decision (in translation), written by Justice Celso Mello, reads:
The right to health — as well as a fundamental right of all individuals — represents an inextricable constitutional consequence of the right to life. . . . The interpretation of a programmatic norm cannot transform it into a toothless constitutional promise . . . Between protecting the inviolability of the right to life, an inalienable fundamental right guaranteed by the Constitution itself (art. 5º, caput) or ensuring, against this fundamental prerogative, a financial and secondary interest of the state, I believe — once this dilemma is established — ethical and legal reasons impose on the judge one single and possible option: unswerving respect for life.13
This expansive interpretation of the right to health, which is now firmly established in all levels of the judiciary, created a favorable environment (or a favorable “opportunity structure for litigation”) for hundreds and then thousands of individual claimants seeking satisfaction of health needs via courts.14 Indeed, all that a claimant must do to win his or her case under this interpretation is to prove that he or she has an unsatisfied health need as documented by a doctor’s prescription.15 Not surprisingly, right-to-health litigation has exploded, spreading from mostly HIV/AIDS-related cases in the late 1990s to several other areas of health in the 2000s, including, for example, diabetes, Parkinson disease, Alzheimer’s, hepatitis C, and multiple sclerosis.16 There is not yet any comprehensive and systematic study that provides a clear picture of the magnitude of the phenomenon in Brazil. But several localized studies and one recent comparative study, together with data released periodically in the press by health authorities, suggest that the phenomenon is widespread, is growing exponentially, and is likely to be reaching (or to have already reached) significant levels in terms of volume and costs.
In their pioneering study, published in 2004, Ana Messeder, Claudia Osorio-de-Castro, and Vera Luiza traced the evolution of right-to-health litigation in the state of Rio de Janeiro from 1991, when they found a single case, to 2002, a year in which 1,144 lawsuits were filed.17 In a later study, in 2007, Danielle Borges found 2,245 cases against the same state in 2005 alone, a growth of almost 350% from 2001 levels.18 This significant growth in health litigation is not a phenomenon restricted to the state of Rio de Janeiro. Florian Hoffman and Fernando Bentes also found a significant and growing number of cases (7,400 from 1995 to 2004) in their comparative study of the states of Rio Grande do Sul, Bahia, Pernambuco, Rio de Janeiro, and Goias.19 Other studies have identified a similar growth in litigation in São Paulo and Santa Catarina.20 All studies without exception report a high prevalence of individual claims (claims brought by or on behalf of single individuals) rather than collective claims (“class actions”) and an extremely high success rate for claimants, ranging from 82% in the lower courts and courts of appeal to almost 100% in the STF.21
The increase of state expenditure to comply with the corresponding court orders further reflects this growth in the number of successful cases. According to data from the Ministry of Health, R$48 million (approximately US$24 million, about 1% of the total federal health budget for medicines) was spent at the federal level in the first seven months of 2008 for the acquisition of medicines ordered by courts. This was three times higher than the expenditure in 2007 and an almost 2,000% increase since 2005. The expenditure is even higher at the level of the states, which are also responsible for guaranteeing the right to health according to the constitution. São Paulo, for instance, the largest in population and the richest state, spent R$300 million (approximately US$150 million) in 2007 alone; Rio Grande do Sul and Minas Gerais, other large states, spent R$78 million (approximately US$39 million) and R$40 million (approximately US$20 million), respectively.22
These numbers show that the Brazilian courts have been interfering with public health policy through right-to-health litigation by issuing daily orders that compel the state to provide drugs and other health treatments to thousands of patients.23 Given the consistent compliance of the Brazilian public health administration with these judicial orders — often not part of the response in other countries experiencing a similar phenomenon — the cumulative effect of these judicial orders can drastically affect the operation of the public health system.24 Budgets and health policy plans must be changed daily, shifting resources from the areas and policies for which they were targeted, in order to cover the new expenditure created by court orders.25 For many, this administrative pandemonium is sufficient reason to conclude that courts should be prevented from adjudicating health and other matters of social and economic policy. I will focus, however, on the potential negative effects that this prevalent Brazilian model of litigation has on health equity.
Defining health equity in the Brazilian context
In order to assess the impact of a phenomenon such as litigation on health equity, it is necessary first to specify what I mean here by health equity, given the lack of broad consensus on its definition. It is important first to note the differences and connections between the ideas of health equality and health equity. Although some writers seem to use both terms interchangeably and to assume that any inequality in health is a health inequity, I support the position of those such as Amartya Sen, who argues that “the violation of health equity cannot be judged merely by looking at inequality in health.”26 Thomas Pogge made a similar point when he wrote that “moral assessment must … be sensitive not merely to the distribution of health outcomes as such, but also to how these outcomes are produced.”27 This definition encompasses most people’s intuition that what is “particularly serious as an injustice is the lack of opportunity that some may have to achieve good health” because of factors beyond their control (such as discrimination and poverty) as opposed to personal free choices not to worry about health (such as a conscious decision to smoke despite knowledge of the health risks involved).28 Goran Dahlgren and Margaret Whitehead expressed this point with the general formulation that “health inequalities count as inequities when they are avoidable, unnecessary, and unfair.”29
The consensus — if there is one as I suggest — stops at this general formulation. What particular instances of health inequality count as avoidable, unnecessary, and, most importantly, unfair is still a matter of great controversy. It is often also impossible, unacceptable (for reasons of privacy, for instance), or undesirable to probe into individuals’ lives to determine whether current health inequalities are a consequence of individual choices or social circumstances beyond individual control.30 We must therefore rely heavily on the more determinate idea of health equality. This is possible since, as Sen observed, “in most situations, health achievement tends to be a good guide to the underlying capabilities [to achieve good health], since we tend to give priority to good health when we have the real opportunity to choose.”31
Where health inequalities are as pronounced as they are in Brazil, one of the most unequal societies in the world, we might assume that these inequalities are at least in part unjust, that is, they are also health inequities. This is illustrated in Table 1.
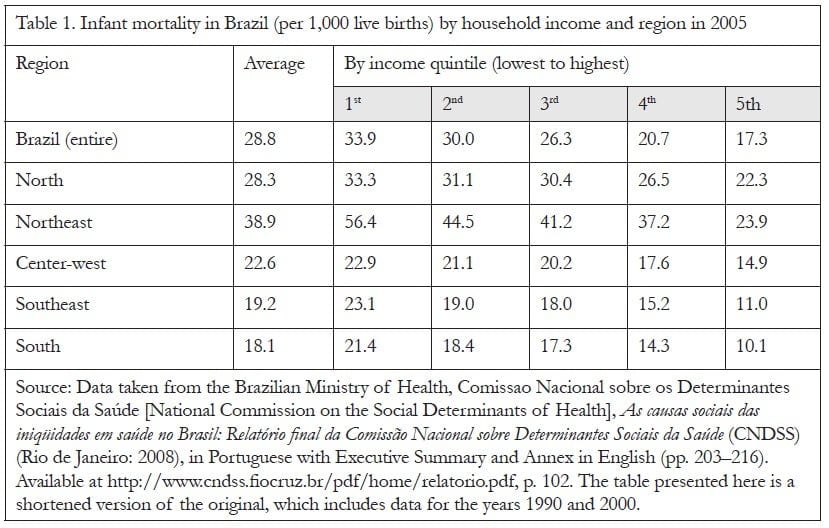
Despite a significant reduction in infant mortality, from a national average of 53.7 per 1,000 live births in 1990 to 28.8 per 1,000 in 2005, Table 1 shows that the infant mortality rate of the poorest 20% of the population, who live in the Northeast, was 56.4 per 1,000 in 2005 (above the country average in 1990), whereas it was 10.1 and 11 per 1,000 for the richest 20% of the population living in the South and Southeast, respectively. The latter figures are closer to the average of developed countries. The same social gradient is evident in all other health indicators, including child mortality and life expectancy.32 Drawing again on Sen’s comment, above, we can assume that the predicament of the majority of the Brazilian population whose health achievement is still so low (and significantly lower than the health achievement of the average and the better off) is mostly due to their lack of real opportunity to achieve good health rather than a personal free choice to disregard their health. In no truly democratic society — where most people have a reasonably wide range of opportunities — would health inequalities (and associated inequalities in wealth and living standards) achieve the levels currently present in Brazil.
Those who framed the 1988 Brazilian constitution accepted this assumption when they included “reducing social and regional inequalities” as one of the main aims of the Brazilian Republic (art. 3, III). The Brazilian constitution is thus expressly transformative and egalitarian.33 It was built on the wide consensus that the pre-constitutional order was unjust, establishing transformative goals that the state and society must strive to achieve. One of these goals is the reduction in inequalities in health. Indeed, before the recognition of health as a constitutional fundamental right, opportunities to achieve health were distributed using market logic, that is, on the basis of the ability to afford social determinants of health and to pay for services offered by private health care providers, funded either directly or indirectly through one’s employer. The constitution ordered the creation of a public health system “free at the point of delivery,” aiming to extend health actions and services to those previously excluded. This is the meaning of “universal access” as it is stated in Article 196 of the constitution:
Health is the right of all and a duty of the State and shall be guaranteed by means of social and economic policies aimed at reducing the risk of illness and other hazards and at the universal and equal access to actions and services for its promotion, protection and recovery.34
Thus, we may assume, at least in the Brazilian context, that the status quo is iniquitous and that the state has a constitutional duty to diminish the vast health inequalities that persist among different socioeconomic groups of the population. Yet given resource limitations and moral disagreement about which health needs should be met, how can “priority — or limit-setting decisions come to be accepted as fair and legitimate?”35 In the Brazilian context, again, we can assume that fair and legitimate decisions should give some priority to the health needs of those at the bottom of the ranking of health achievement, historically disadvantaged by the socioeconomic-political system.
One must still define with more precision how far health inequalities should be diminished and how much priority should be given to the most disadvantaged. Nevertheless, the generic aims summarized above help us to assess any measure or practice, such as a state health program or the “Brazilian litigation model,” in light of these aims. That is, we can profitably assess whether or not a measure or practice gives any priority to the worse off and if, in doing so, it tends to diminish the country’s pronounced health inequities.
Take, for example, two government programs in Brazil that are highly regarded internationally, the Programa Nacional DST/AIDS (the National HIV-AIDS Program) and the Programa Saúde da Família (or Family Health Program). The Programa Nacional DST/AIDS provides free treatment for HIV/AIDS (and, to a much lesser scale, other sexually transmitted diseases) to around 135,000 individuals, including free provision of antiretroviral drugs.36 In 2006, its budget was R$1.3 billion (approximately US$650 million, almost 80% for purchasing drugs).37 The Programa Saúde da Família is a strategy for reorganizing primary health care by focusing on preventive action. It establishes multidisciplinary health care teams, comprised of physicians, nurses, community health workers, and oral health professionals, who are responsible for meeting the basic health care needs of a specified number of households in a specified area. In 2006, the Programa Saúde da Família served around 82 million people (almost half of the Brazilian population), at the cost of R$2 billion (approximately US$1 billion).38 Both programs can be assessed from the perspective of health equity outlined above and are examples of it. Indeed, some have claimed that the Programa Nacional DST/AIDS worsens health equity by focusing on expensive drugs for a disease that in Brazil often affects comparatively more individuals from higher socioeconomic groups.39 On the other hand, it is argued that the Programa Saúde da Família, by focusing on preventive action against health problems that affect comparatively more individuals from lower socioeconomic groups, improves health equity. 40 Without more detailed exploration of either these assertions or the controversies that they raise, I suggest that these programs illustrate how a measure or a practice can be usefully assessed in terms of its impact on health equity, even if we do not yet possess a broadly agreed-upon and precise specification of the meaning of the term.
The impact of the Brazilian model on health equity
Does the Brazilian model of litigation give priority to the health needs of those at the bottom of the ranking of health achievement, consequently diminishing the vast health inequalities that persist in the country? In order for the model to have this effect, the majority of litigants would need to belong to the lower socioeconomic groups of Brazilian society, such as the first and second quintiles of income shown in Table 1.41 But this is not the case. Access to the courts in Brazil (as in most places) is significantly easier for those with resources and social attributes that are more predominant in higher socioeconomic groups. Such resources and attributes, to quote Siri Gloppen, include “rights awareness; organizational strength and ability to mobilize; and access to legal assistance, technical expertise, and financial resources.”42 Several recent empirical studies on the phenomenon of health litigation confirm, predictably, that a significant portion of successful litigants do not belong to the most disadvantaged layers of society, but rather the opposite.
Indirect indicators: Legal representation and health services used
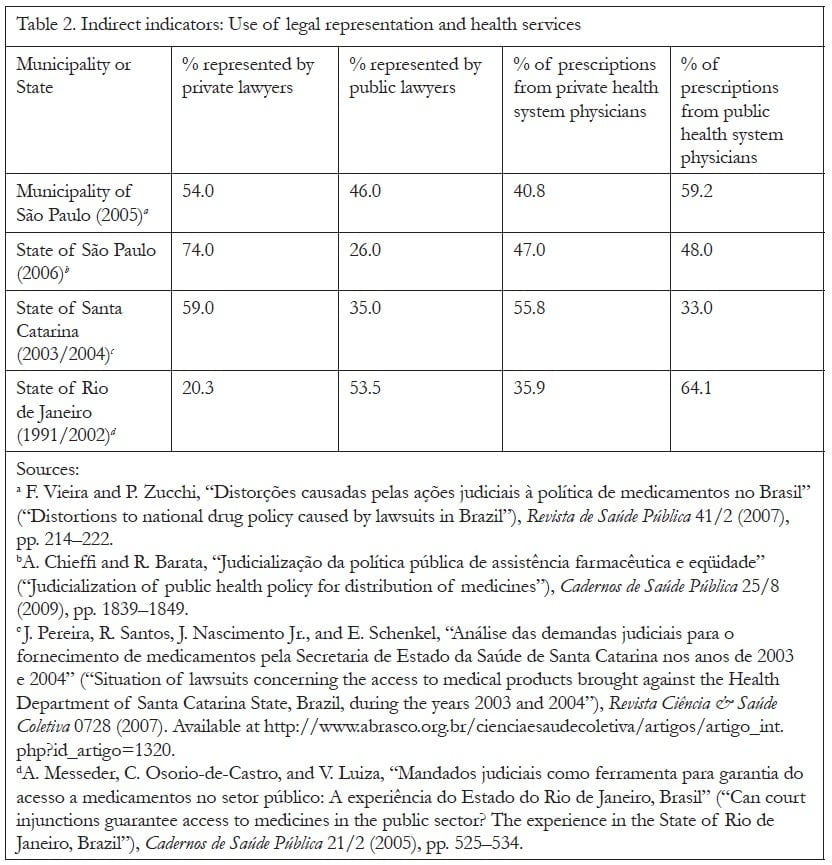
The two most common indirect indicators of litigants’ socioeconomic status are the type of legal representation used by claimants (private vs. public legal services) and the origin of the medical prescription that supports the claim (public vs. private health services). The plausible assumption is that representation by a private lawyer and use of the private health system, especially when they occur together, would strongly indicate a high socioeconomic profile of the litigant.43 Indeed, given that the two poorest quintiles of the Brazilian population, that is, cumulatively the poorest 40%, have an average monthly per capita income of 0.42% of the minimum wage, it is unlikely that they would be able to afford the services of private lawyers and doctors.44 Table 2 compiles information on the use of private and public legal and health services available from studies conducted in the municipality of São Paulo and in the states of São Paulo, Rio de Janeiro, and Santa Catarina.
As Table 2 shows (see next page), all studies to date except one demonstrate that the majority of claimants are represented by private lawyers, and a significant percentage of prescriptions originate in the private health system.45 The exception is an early study of litigation in the state of Rio de Janeiro.46 Yet one must not assume that this study indicates that, at least in Rio de Janeiro, litigation is benefiting the worst off and improving health equity. Although most claimants represented by public lawyers are indeed often comparatively worse-off than those represented by private lawyers, public representation does not mean that the claimants come from the lowest income quintiles of the Brazilian society.47 On the contrary, factors such as flexible means criteria for qualifying for public legal services, higher rights awareness, office location, and available transportation lead an increasing number of middle-class claimants to be represented by public lawyers, especially in cases involving expensive medication.48 In a recent study of litigation in the state of São Paulo, for example, Daniel Wang found that the median household income of claimants represented by public lawyers from June 2008 to January 2009 was just below the minimum salary.49 That is, more than half of the claimants were above that level, and thus did not represent the two lowest quintiles of the population.50 In another study, it was observed that the public lawyers’ offices in the state of Bahia are located in a middle-class district that is difficult to access by public transportation.51
The higher prevalence of prescriptions issued by physicians of the public system in the Rio de Janeiro study should also be interpreted with caution. Whereas the poorest patients will rarely use private doctors, it is not difficult for richer patients to occasionally use the public system, for instance to get a prescription to support a judicial claim.52
Direct indicators: Residence, income, and education
More precise information on the socioeconomic profile of claimants can be gathered through direct indicators such as residence, income, and education. A few studies have used innovative methods to gather this information. Fabiola Vieira and Paola Zucchi, for instance, analyzed claimants’ addresses and found that 63% in their sample lived in the areas of the city with the lowest levels of social exclusion.53 In a more recent study, Ana Chieffi and Rita Barata used the São Paulo Index of Social Vulnerability (which divides the city into six homogenous areas) and found that 74% of the claimants lived in the three areas with the lowest social vulnerability rates.54 Fernanda Terrazas confirmed these findings by interviewing a random sample of 160 successful claimants in the state of São Paulo.55 Over 70% stated that they lived in their own house in an upper-class, middle-class, or lower-middle-class neighborhood, and more than 58% stated that they lived in households with an income over the minimum wage per capita. A significant percentage of respondents had incomes well above that level, with 23.75% reporting incomes two to five times the minimum wage and with 11.8% reporting an income more than five times the minimum wage. Perhaps more striking, over 80% of Terrazas’ sample had completed secondary education or higher, whereas in 2006, only 39.2% of the state’s population had completed this level of education.56
Conclusion
The emerging evidence gathered in the available studies on right to health litigation conducted in Brazil indicates that a significant proportion of litigants do not come from the most disadvantaged socioeconomic groups in society. For many, these findings are notable but not surprising. They are also consistent with other studies, such as the recent comparative study by Gauri and Brinks of social rights litigation in Asia, Africa, and Latin America. Such research shows that the direct effects of litigation benefit predominantly those individuals “in the middle of the social spectrum,” that is, “neither the most disadvantaged nor the wealthiest citizens.”57
It is clear, thus, that the model of litigation currently prevalent in Brazil is not improving health equity. But does it worsen health inequities? I suggest that it does, although the extent to which this occurs is difficult to determine with any precision without further research on the opportunity costs of such litigation. It is likely that the increasing amount of resources spent to fund the health benefits granted to successful claimants (hundreds of millions of dollars in some states, mostly consumed to purchase expensive new drugs) is diverted at least in part from current or future health programs that would benefit larger and more disadvantaged groups who cannot easily access the courts to protect their interests. Take as an example the case of the state of São Paulo, where data is more easily available and comprehensive. In 2008, the state spent approximately R$400 million (approximately US$200 million) to comply with court orders benefiting around 35,000 successful claimants, mostly to purchase expensive drugs, many of which have to be imported and are not even registered for use in Brazil.58 This is roughly the same level of resources that the federal Ministry of Health has recently announced will be invested in a program of vaccination against pneumococcal bacteria to cover all 3.2 million children born every year in Brazil. But this program will not be fully implemented until 2010 due to resource limitations of the health budget.59 Further research on the opportunity costs of right-to-health litigation will be very important in assessing health equity.
Whether this model of litigation can be changed or is deeply ingrained in the Brazilian (and also other countries’) legal culture remains an important and complex issue. Some claim, for instance, that an effort can be made so that more disadvantaged individuals have access to the courts.60 Others argue that the right to health should be claimed only collectively, via class actions sponsored by public lawyers on behalf of large groups of disadvantaged individuals.61 While further discussion on this issue is beyond the scope of this paper, I suggest that the main problem lies elsewhere, that is, in the current dominant interpretation of the right to health by Brazilian courts as an individual entitlement to the satisfaction of all one’s health needs with the most advanced treatment available. This can only be sustained at the cost of universality, whoever manages to reach the courts, since only a minority of individuals (irrespective of whether they are rich or poor) would ever be able to enjoy this expansive (and expensive) right at any given time within a context of necessary resource limitations. Given these limits, the problem would not be solved if access to the judiciary were extended to the most poor, but would rather be magnified beyond manageable proportions. Such a consequence might be a positive development under the present circumstances. It would force courts and supporters of the current interpretation of the right to health to see that the right to health must be interpreted as a right to equal access to health actions and services that can be provided within available resources. But given that full access to courts for the most poor is a rather unlikely development, we need to find some other speedier and less dramatic route to highlight the basic flaws and perverse effects on health equity of the current model. I hope this article might contribute to that endeavor.
Acknowledgment
An earlier version of this paper was presented in a seminar at Universidad Torcuato Di Tella, Buenos Aires, in early 2009. I am grateful to all the participants for an invaluable debate and to Alicia Ely Yamin, the HHR editors, and anonymous referees for helpful comments on earlier drafts. Some of the data was gathered as part of the Chr. Michelsen Institute (University of Bergen, Norway) project, “The right to health through litigation? Can court-enforced health rights improve health policy?” and funded by the Research Council of Norway (GLOBVAC).
References
1. J. J. Rousseau, Discours sur l’économie politique (1755). Available at http://classiques.uqac.ca/classiques/Rousseau_jj/discours_economie_politique/discours_eco_pol.html.
2. U. Baxi, “The Avatars of Indian Judicial Activism,” in S. K. Verma and Kusum (eds), Fifty years of the Supreme Court of India: Its grasp and reach (New Delhi: Oxford University Press, 2000), p. 161.
3. For a good account of the history, successes, and failures of the “sanitary movement” into the mid-1990s, see K. Weyland, “Social movements and the state: The politics of health reform in Brazil,” World Development 23/10 (1995), pp. 1699–1712.
4. Ibid., p. 1703.
5. For the most comprehensive and up-to-date analysis of health inequalities in Brazil, see National Commission on Social Determinants of Health, As causas sociais das iniqüidades em saúde no Brasil: Relatório Final da Comissão Nacional sobre Determinantes Sociais da Saúde (CNDSS) (Rio de Janeiro: Brazilian Ministry of Health, 2008), in Portuguese with an Executive Summary and Annex in English (pp. 203–216). Available at http://www.cndss.fiocruz.br/pdf/home/relatorio.pdf.
6. J. Lambert, Os dois Brasis (Brasilia: INEP, 1959).
7. K. Weyland, Democracy without equity: Failures of reform in Brazil (Pittsburgh, PA: University of Pittsburgh Press, 1996).
8. I have dealt in some detail with these issues in O. Ferraz, “Poverty and human rights,” Oxford Journal of Legal Studies 28/3 (2008), pp. 585–603, and in O. Ferraz, “Between usurpation and abdication? The right to health in the courts of Brazil and South Africa,” Social Science Research Network (August 20, 2009). Available at http://ssrn.com/abstract=1458299.
9. Three very recent decisions by the president of the STF seem to signal a potential change in the current jurisprudence, but it is too early to tell. For a summary, see “Presidente do STF decide ação sobre fornecimento de remédios com subsídios da audiência pública sobre saúde.” Available at http://www.stf.jus.br/portal/cms/verNoticiaDetalhe.asp?idConteudo=113461.
10. See R. G. Parker, J. Galvão, and M. S. Bessa (eds), Saúde, desenvolvimento e política: Respostas frente à AIDS no Brasil (São Paulo: Editora 34, 1999), p. 11.
11. For a brief account of the historical development of right-to-health litigation in Brazil, see Brazilian Ministry of Health, O remédio via justiça: Um estudo sobre o acesso a novos medicamentos e exames em HIV/AIDS no Brasil por meio de Ações Judiciais (Brasilia: Ministry of Health, 2005).
12. Until very recently, the Brazilian system had no binding precedents. Each judge at any level was able to decide freely each new case, even if the STF had already decided thousands of similar cases in a particular way. That had an important effect on the number of cases coming to courts. This changed with the reforms that occurred in late 2006 (brought about by Federal Laws 11.417 and 11.418); the STF is now able to issue “binding principles” (sumulas vinculantes) with erga omnes effect whenever it feels that an issue has been thoroughly analyzed and decided in a certain way several times. No binding principle has been issued on right-to-health litigation to date, although the STF is presently considering this option. Unless otherwise noted, all translations of Brazilian legal terms and documents cited in this paper are by the author.
13. RE 271.286 AgR- RS (2000), Relator Min. Celso de Mello. Translated from the Portuguese at the STF website (http://www.stf.gov.br/), where the original reads: “O direito à saúde — além de qualificar-se como direito fundamental que assiste a todas as pessoas — representa conseqüência constitucional indissociável do direito à vida. … A interpretação da norma programática não pode transformá-la em promessa inconsequente. … Entre proteger a inviolabilidade do direito à vida, que se qualifica como direito subjetivo inalienável assegurado pela própria Constituição da República (art. 5º, caput), ou fazer prevalecer, contra essa prerrogativa fundamental, um interesse financeiro e secundário do Estado, entendo — uma vez configurado esse dilema — que razões de ordem ético-jurídica impõem ao julgador uma só e possível opção: o respeito indeclinável à vida.”
14. The phrase “opportunity structure for litigation” is from S. Gloppen, “Litigation as a strategy to hold governments accountable for implementing the right to health,” Health and Human Rights: An International Journal 10/2 (2009), pp. 21–36.
15. It is important to note that a minority of judges in the lower courts and courts of appeal of several states still decide against claimants on the basis that the best interpretation of the right to health does not mean unlimited access to medical treatment, but rather a right to equal access to health benefits the state is able to provide within limited resources. This explains why (as mentioned later in the text) the rate of success in right-to-health litigation is not 100%.
16. Brazilian Ministry of Health (see note 11). It is important to note here, however, that not all decisions of that period concerned HIV/AIDS treatment. In fact, in what is probably the earliest decision favoring a patient by the STF, the case concerned an individual suffering from Duchenne muscular dystrophy whose treatment in the US was funded through an interim first instance court order upheld by the STF in AgrPet 1246–1— SC (1997).
17. A. Messeder, C. Osorio-de-Castro, and V. Luiza, “Mandados judiciais como ferramenta para garantia do acesso a medicamentos no setor público: A experiência do Estado do Rio de Janeiro, Brasil” (Can court injunctions guarantee access to medicines in the public sector? The experience in the State of Rio de Janeiro, Brazil), Cadernos de Saúde Pública 21/2 (2005), pp. 525–534.
18. D. Borges, Uma análise das ações judiciais para o fornecimento de medicamentos no âmbito do SUS: O caso do Estado do Rio de Janeiro no ano de 2005, MPhil thesis (Fiocruz, 2007). Available at http://bvssp.icict.fiocruz.br/lildbi/docsonline/3/3/1233-borgesdclm.pdf.
19. F. Hoffman and F. Bentes, “Accountability for social and economic rights in Brazil,” in V. Gauri and D. Brinks (eds), Courting social justice: Judicial enforcement of social and economic rights in the developing world (Cambridge, UK: Cambridge University Press, 2008), pp. 100–145.
20. For a review of studies surveying right-to-health litigation, see O. Ferraz, “Right-to-health litigation in Brazil: An overview of the research” (presentation at The Right to Health through Litigation? Can Court Enforced Health Rights Improve Health Policy? (workshop), Universidad Torcuato Di Tella, Buenos Aires, April 15–17, 2009). Available at http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1426011. A recent search in the database of the São Paulo Court of Appeals (one of the 27 courts of appeal of Brazil) for the terms equivalent to “right to health” and “medicines” retrieved 6,617 decisions in 2008 alone, all of which were individual claims. I thank Daniel Wang for this data.
21. For an analysis of 48 decisions by the STF, all of them successful for the litigant, see M. Barbosa, “O STF e a política de fornecimento de medicamentos para tratamento de AIDS/HIV,” in D. Coutinho and A. Vojvodic (eds), Jurisprudência Constitucional: Como decide o STF? (São Paulo: Malheiros, 2009), pp. 335–350.
22. C. Collucci, “Triplicam as ações judiciais para obter medicamentos,” Folha de S. Paulo (January 9, 2009).
23. The involvement of Brazilian courts, in particular the STF, in areas traditionally regarded as political has grown across the board. Health is only one of them, and even within health litigation for medical treatment is one among many others, such as recent controversial cases like stem cell research and abortion of anencephalic fetuses. For an academic treatment of the general phenomenon, see M. Taylor, Judging Policy: Courts and Policy Reform in Democratic Brazil (Stanford, CA: Stanford University Press, 2008).
24. For a recent comparative study of countries in Africa, Asia, and Latin America with data on compliance with court orders, see Gauri and Brinks (see note 19).
25. See F. Vieira and P. Zucchi, “Distorções causadas pelas ações judiciais à política de medicamentos no Brasil” (Distortions to national drug policy caused by lawsuits in Brazil), Revista de Saúde Pública 41/2 (2007), pp. 214–222, and Messeder, Osorio-de-Castro, and Luiza (see note 17).
26. A. Sen, “Why health equity?” in S. Anand, F. Peter, and A. Sen (eds), Public Health, Ethics, and Equity (Oxford: Oxford University Press, 2006), p. 25.
27. T. Pogge, “Relational Conceptions of Justice: Responsibility for Health Outcomes,” in Anand, Peter, and Sen (see note 26), pp. 135–161, at p. 135.
28. Sen (see note 26), p. 25.
29. As cited in N. Daniels, Just health: Meeting health needs fairly (New York: Cambridge University Press, 2008), p. 89.
30. See, for this argument, R. Arneson, “Egalitarian justice versus the right to privacy,” Social Philosophy and Policy 17/2 (2000), pp. 91–119.
31. Sen (see note 26).
32. Ibid. See also M. Barreto and R. Aquino, “Recent positive developments in the Brazilian health system,” American Journal of Public Health 99/1 (2009), p. 8.
33. For the idea of transformative constitutionalism see S. Liebenberg, Needs, rights, and transformation: Adjudicating social rights, NYU Center for Human Rights and Global Justice Working Paper 8 (New York: New York University, 2005). Available at http://www.chrgj.org/publications/docs/wp/Liebenberg%2020Needs,%20Rights%20and%20Transformation.pdf.
34. Bazilian 1988 Constitution, English version, from the Political Database of the Americas, Center for Latin American Studies, Georgetown University, November 2008. Available at http://pdba.georgetown.edu/Constitutions/Brazil/english96.html#mozTocId339966.
35. Daniels (see note 29).
36. J. Galvao, “Brazil and access to HIV/AIDS drugs: A question of human rights and public health,” American Journal of Public Health 95/7 (2005), pp. 1110–1116.
37. P. Mazenotti, “Programa DST/Aids usou quase todos os recursos previstos para 2005, diz diretor” (January 5, 2006). Available at http://www.direitos.org.br/index.php?option=com_content&task=view&id=753&Itemid=1.
38. R. Aquino, N. de Oliveira, and M. Barreto, “Impact of the Family Health Program on infant mortality in Brazilian municipalities,” American Journal of Public Health 99/1 (2009), pp. 87–93; for the costs and population served, see National Commission on Social Determinants of Health (see note 5), p. 67.
39. P. Lotufo, “Coffee, samba, football and … inequalities: Reflections on mortality in São Paulo, Brazil,” São Paulo Medical Journal/Revista Paulista de Medicina 119/3/9 (2001), pp. 4–6. Available at http://www.scielo.br/scielo.php?pid=S1516-31802001000300001&script=sci_arttext; and M. Drumond and M. Barros, “Desigualdades socioespaciais na mortalidade do adulto no Município de São Paulo / Social inequalities in adult mortality in the City of S. Paulo,” Revista Brasileira de Epidemiologia 2/1–2 (1999), pp. 34–49. Available at http://www.scielo.br/pdf/rbepid/v2n1-2/04.pdf.
40. Aquino, de Oliveira, and Barreto (see note 38).
41. Additional conditions should also be present. The health benefits claimed in court would have to be of a kind that effectively diminish health inequities (for example, primary attention and social determinants), and the resources to fund these benefits would have to either come from additional investment in health or be diverted from health programs that benefit higher socioeconomic groups, such as the fourth and fifth quintiles of income. There is some indication that neither of these conditions applies, but this will not be discussed in any length here given that the first necessary condition (that is, the socioeconomic profile of litigants), for which there is stronger evidence as discussed in the text, does not apply.
42. Gloppen (see note 14), p. 28; Gauri and Brinks (see note 19), pp. 336–337.
43. Around 41 million Brazilians were covered by private health insurance at the end of 2008 (21.1% of the population), according to the official data of the Agência Nacional de Saúde Suplementar (ANS), the organization that regulates private health care in Brazil, available at http://www.ans.gov.br/portal/site/informacoesss/iss_dados_gerais.asp. Although some workers have their insurance funded by employers, very few of these individuals will likely be in the lower two quintiles of income, where most individuals are either unemployed, employed in the informal sector, or have very low-paid jobs that are unlikely to include private health insurance (see note 44).
44. Brazilian Institute of Geography and Statistics (IBGE), Síntese de Indicadores Sociais — 2007. Available at http://www.ibge.gov.br/home/presidencia/noticias/noticia_impressao.php?id_noticia=987; see especially Fig. 4.4.
45. This pattern was also found in S. Marques and S. Dallari, “Garantia do direito social à assistência farmacêutica no Estado de São Paulo” (“Safeguarding of the social right to pharmaceutical assistance in the state of São Paulo, Brazil”), Revista de Saúde Pública 41/1 (2007), pp. 101–107; and F. Terrazas, O Poder Judiciário como voz institucional dos pobres: O caso das demandas judiciais por medicamentos, MPhil thesis (University of São Paulo, 2008).
46. Messeder, Osorio-de-Castro, and Luiza (see note 17).
47. By “public lawyers,” I mean two different groups of lawyers paid by the state: defensores públicos (“public defenders), whose duty is to represent claimants unable to afford private legal services, and promotores públicos (“public promoters”), whose duty is broader, including the defence of so-called public and diffuse interests, such as the environment, the economic order, and architectural heritage.
48. Hoffman and Bentes (see note 19), pp. 112–113 and p. 142.
49. D. Wang, Poder Judiciário e participação democrática nas políticas públicas de saúde, MPhil thesis (University of São Paulo, 2009), p. 83.
50. The same was found by J. Sant’ana, Essencialidade e assistência farmacêutica: Um estudo exploratório das demandas judiciais individuais para acesso a medicamentos no estado do Rio de Janeiro, MPhil thesis (Fiocruz, 2009).
51. Hoffman and Bentes (see note 19), p. 113.
52. As has occurred in São Paulo during a brief period in which some lower court judges started to condition successful claims on the presentation of a public doctor’s prescription; interview with Adriana Daidone, a private attorney in São Paulo who represents hundreds of individual claimants in right-to-health litigation (July 29, 2009). See also A. Chieffi and R. Barata, “Judicialização da política pública de assistência farmacêutica e eqüidade” (“Judicialization of public health policy for distribution of medicines”) Cadernos de Saúde Pública 25/8 (2009), pp. 1839–1849.
53. Vieira and Zucchi (see note 25).
54. Chieffi and Barata (see note 52).
55. Terrazas (see note 45).
56. In Terrazas’s sample (see note 45), 25% had completed higher education, and 5.63% held postgraduate degrees. For data on the educational level of the population as a whole, see São Paulo State Government, Pesquisa Condicoes de Vida 2006 (São Paulo: Fundacao SEADE, 2006). Available at http://www.seade.gov.br/produtos/pcv/pdfs/escolaridade.pdf.
57. Gauri and Brinks (see note 19), pp. 336–337. They also suggest, very tentatively, that the indirect effects of litigation (for example, via changes in health policy) might have a higher potential to benefit less advantaged individuals. For the reasons mentioned in the main text, I am highly skeptical of this possibility.
58. Interview with Maria Cecilia Correa, public health expert in the São Paulo State Health Department, coordinator of the right-to-health litigation unit (CODES), (July 22, 2009).
59. D. Menchen, “SUS vacinará contra pneumococo em 2010,” Folha de S. Paulo (August 18, 2009).
60. Wang (see note 49).
61. For this suggestion, see Hoffman and Bentes (see note 19), p. 145. They also discuss in their research the possible explanations for the insignificant number of such type of actions at present.