Taking up Daniels’ challenge: The case for global health justice
Gorik Ooms and Rachel Hammonds
Health and Human Rights 12/1
Published June 2010
Abstract
In Just Health, Norman Daniels makes a strong argument for obligations of mutual assistance to fulfill the right to health at the national level and challenges readers to develop arguments supporting obligations of mutual assistance at the global level. In this paper, we argue that there is global responsibility for global health and that there are obligations of justice (beyond charity) to help fulfill (not merely respect or even protect) the right to health in other countries; these we call obligations of global health justice. We show how international human rights law affirms obligations of global health justice — beyond national obligations and beyond obligations of charity — and assert that the human rights approach provides guidance on delineating the relationship between national and global responsibility for fulfilling the core obligations that arise from socioeconomic human rights and addressing global health inequities. We further argue that new ways of providing international assistance, originating from the global HIV/AIDS response, demonstrate the feasibility of improving health outcomes through exogenous efforts and that obligations of global health justice thus carry much weight: the weight of lives not saved. The global response to the HIV/AIDS pandemic has led to the emergence of a new international health assistance paradigm, and the Global Fund to fight AIDS, Tuberculosis and Malaria is, we suggest, an embryonic form of this new paradigm. We conclude that agreements on several common parameters delineating global and national responsibility for global health can advance the movement towards a global institution for the distribution of health-related goods.
Introduction
In his book, Just Health, Norman Daniels develops a complex theory of health justice with a call for action.1 While making a strong case for national health justice (a case for obligations of mutual assistance to reduce health inequalities at the national level), Daniels wonders whether he can stretch his theory to also make the case for obligations of mutual assistance beyond state borders. Daniels acknowledges that arguments of relational justice, on which his theory of health justice is based, cannot easily be expanded to the global level. Yet he notes in his “concluding challenge” that, “[d]espite the lack of closure on these matters, the account developed here provides an integrated theory that helps us see the path to pursue in promoting population health and distributing it fairly, globally as well as domestically.”2
In this paper, we take up Daniels’ challenge for action. Building on several of his arguments, we apply his framework to further develop a thesis we have published elsewhere concerning global responsibility for health.3 We understand such global responsibility as supplementing, not replacing, national responsibility for health.
Daniels’ presentation of the differences between global and national responsibilities in health justice suggests an innate tension, with the path to a successful integration being one that requires careful, constant negotiation between dangerous but opposing alternatives. Throughout this paper we envision the space between these alternatives — the space in which to formulate and establish global health justice — as comparable to the narrow strait between Scylla and Charybdis, the two great sea monsters that Odysseus, in Greek mythology, had to keep equally distant to ensure the safety of his journey through the strait; even when equidistant, the nearness of each threatened to destroy his ship and its sailors.4 Although Daniels does not use the Scylla-Charybdis metaphor directly, his “concluding challenge” is explicitly shaped by an argument that directs the reader to an “intermediary ground” that “resists the pull” of two opposing alternatives. Specifically, he writes:
[I]nquiry should focus on a middle ground between strongly statist claims that egalitarian requirements of social justice are solely the domain of the nation-state and its well-defined basic structure [as drawn from John Rawls and Thomas Nagel] and strong cosmopolitan claims that principles of justice apply to individuals globally, regardless of the relations in which they stand or the institutional structures through with they interact.5
We agree with Daniels on the risks of both of these claims. We agree with his call to resist “the pull of cosmopolitan intuition” since, as he argues, too much focus on global responsibility, without a strong affirmation of the primacy of national responsibility, could erode the latter.6 We also agree that the global institution necessary to govern the relationship between national and global responsibility is lacking, and we argue that this deficiency should provide sufficient impetus to create such an institution. We also agree that it is, at the same time, essential to resist what Daniels calls “strongly statist versions of relational justice.”7 Indeed, if states were the only institutions that could govern health justice, the absence of a “global state” would exonerate states from all responsibility for the consequences of their behavior beyond their immediate national borders.
We disagree with Daniels, however, in his rejection of international human rights law as a potential compass that could guide the journey through this narrow strait of delineating the relationship between national and global responsibility for health. In this paper, we demonstrate how a human rights approach provides guidance for such a journey. We also argue that it is not difficult to perceive what a global institution that could govern this relationship might look like; in fact, we believe a prototype already exists in the form of the Global Fund to fight AIDS, Tuberculosis and Malaria (the Global Fund). The Global Fund structure is presently defined more by its practical action than by any pre-determined theoretical foundation of global health justice. Envisioning the Global Fund as a model useful for giving shape to Daniels’ challenge can also, in turn, provide a theoretical foundation to strengthen the work of the Global Fund itself.
Global responsibility for growing health inequalities
Daniels defines health inequity (or injustice) as the “unjust distribution of the socially controllable factors affecting population health and its distribution.”8 Following John Arras and Elizabeth Fenton, we will here discuss “health-related goods” as shorthand for Daniels’ “socially controllable factors affecting population health and its distribution.”9
Health-related goods cost money. No matter which priorities ranking one uses, health care, prevention, water, sanitation, and nutrition all cost money. Therefore, wealth inequalities between nations have a direct impact on their respective health inequalities. What governments can spend on the distribution of health-related goods depends on their revenue, which is affected by their wealth. The increase in wealth inequality between nations, with its direct effect on health inequity is, we argue, a matter of global responsibility.
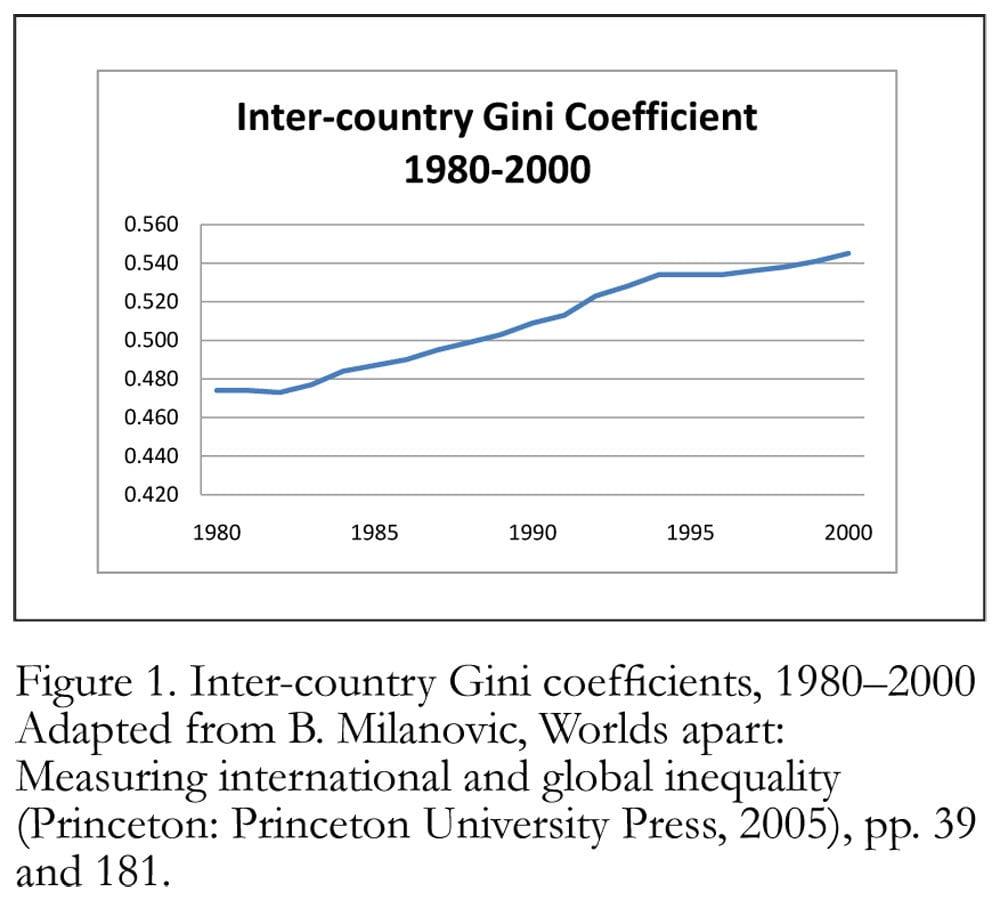
In his studies on the evolution of global wealth inequalities, Branko Milanovic demonstrated that wealth inequalities between countries, expressed as an inter-country Gini coefficient, are steadily growing.10 A Gini coefficient of zero for inter-country wealth distribution would mean that all countries have exactly the same average Gross Domestic Product (GDP) per capita, that is, full inter-country equality. A Gini coefficient of one for inter-country wealth distribution would mean that one single country would enjoy the entire GDP of the world’s economy (or maximum inequality). Figure 1 illustrates how wealth inequality between countries is in fact progressively moving toward maximum inequality and away from maximum equality.
There are many reasons for this increasing inter-country inequality. One that we should not underestimate is the long-lasting effects of slavery and colonization.11 Rich countries use their economic and political power to negotiate uneven trade agreements.12 The shift of financial resources from poor to rich countries that can be attributed to identifiable illegal or at least illicit causes, that is, “illicit financial flows,” also contribute to and can obscure international assistance from rich to poor countries.13
Another cause that can also explain this principle, but may be easily overlooked, is what Robert Merton called the “Matthew Effect.”14 Referring to a verse in the biblical Gospel of Matthew — “For to all those who have, more will be given, and they will have an abundance; but from those who have nothing, even what they have will be taken away” — Merton explains how scientists who already have a well-established reputation in their field are more likely to be recognized and awarded for their work than lesser-known scientists, even when both contribute evenly to a scientific advancement.15
Gunnar Myrdal drew on this same biblical quotation to explain his theory of “circular and cumulative causation,” which predicts growing inequalities within and between countries participating in a free market.16 Myrdal’s theory argues “that the play of the forces of the market normally tends to increase, rather than decrease, the inequalities between regions.”17 Centers of strong economic growth attract capital and skills, and can invest in an efficient logistical infrastructure, thus growing even faster. In their direct periphery, they may cause “spread effects,” that is, benefits for regions that are within the direct periphery of economic growth centers. Further from the center, however, the existence of these “economic growth centers” cause “backwash effects,” as distant regions suffer from the flight of their capital and skills toward economic growth centers. Within wealthy countries, spread effects can be stronger than backwash effects, and “state policies have been initiated which are directed toward greater regional equality: the market forces which result in backwash effects have been offset, while those resulting in spread effects have been supported.”18 Poor countries, on the other hand, tend to predominantly suffer the backwash effects from economic growth centers, since such growth centers are usually located in other countries. In Myrdal’s words:
If from one point of view the explanation of the existing and ever-increasing international inequalities is the cumulative tendency inherent in the unhampered play of the market forces in a situation where the effectiveness of the spread effects is weak, from another point of view the explanation is the absence of a world state which could interfere in the interest of equality of opportunity.19
The impact of obvious global wrongdoings — like colonization and slavery, unfair trade rules, and illicit financial flows — should not be underestimated. In his overview of the many ways in which rich countries are contributing to both the continued poverty of poor countries and poverty within poor countries, Thomas Pogge argued that obligations of global justice are first and foremost obligations of correction to compensate for failure to fulfill the negative duty of doing no harm.20 We also would affirm the critical importance of correcting the obvious harm that is being done by rich countries to the rest of the world. But even if it were possible to correct or compensate for all past and present obvious wrongdoings, even if a level playing field could be established for global free trade, global free trade would still produce some winners and some losers. And if winners are allowed to invest their present gains in future comparative advantages without global corrective measures, the Gini coefficient for inter-country wealth inequality will continue to grow toward one and away from zero. This global-level Matthew Effect is a less obvious form of harm and might therefore not call for correction on the basis of the negative duty of doing no harm. It does call for correction, however, because it reduces some countries’ capacity to distribute health-related goods; as Daniels argues, for obligations of mutual assistance at the national level, “health is of special moral importance because protecting normal functioning helps to protect the range of opportunities open to people and because various theories of justice support the idea that we have an obligation to protect opportunity and thus health.”21 To protect equal opportunity globally, taking the Matthew Effect into account at the global level, obligations of mutual assistance beyond borders are needed.
If health injustice is, as Daniels defines it, the “unjust distribution of the socially controllable factors affecting population health and its distribution,” then one should seriously consider whether or not the global free market — and the growing inter-country wealth inequalities it is producing — is a source of growing health inequalities, insofar as it undermines the ability of poor countries to purchase health-related goods for its inhabitants.22 On this point, one could argue that if the Matthew Effect is inherent to the global free market, the only alternative would be to move away from this system and aim instead for a global multi-state-controlled market. If such a move took place, one could argue, the cure might be worse than the disease. We suggest that there is another alternative.
According to Robert Archer, the dynamic of self-amplifying wealth and poverty was recognized and understood by industrialized countries more than a century ago, when “many governments in richer countries came to realise, or were pressured to accept, that extreme social and economic inequities were unsustainable.”23 To overcome these inequalities, Archer asserts that “systems of universal health care, social security, unemployment insurance and public housing were put in place.”24 These systems, known as social protection schemes, have been invented and reinvented repeatedly, and they take many different shapes and forms. But in essence, they all effect similar actions: financial resources are collected in accordance with participants’ means and redistributed directly or in the form of health-related goods, education-related goods, or other social rights related goods, in accordance with participants’ needs. The primary distribution of wealth, resulting from free markets, did not guarantee the just distribution of these goods. A secondary system for wealth redistribution was needed, through redistribution that involved either money transfers or social rights-related goods transfers (such as, for example, the government purchasing health care services for individuals who need it).25 As we argue further below, a similar system of secondary redistribution of wealth at the global level could successfully counter the Matthew Effect and allow a less unjust distribution of health-related goods to take place. It is precisely because a secondary redistribution of wealth system fails to occur at the global level, as Myrdal notes, that we argue for the need to recognize and support global responsibility for growing health inequalities. In short, we do not argue that the global free market ought to be abolished but rather that it be adjusted to address and correct this distortion.
Global ability to redress growing health inequalities
Daniels emphasizes that some developing countries perform much better than others when it comes to improving the health of their population, and therefore that the “[p]rimary responsibility for realizing rights to health and health care in a population should rest with each state.”26 We would agree, as long as this statement is not misunderstood to suggest that the secondary global responsibility is meaningless. Indeed, given the rather disappointing track record of global efforts to improve global health, it is tempting to conclude that real progress in reducing health inequalities can only come from endogenous efforts.27 But perhaps the partial failure of exogenous efforts is a result of lack of effort due precisely to the conviction that endogenous activities are the key to real progress in global health.
This misperception is evident in the way that sustainability is commonly viewed. In the field of international assistance for health, according to Enrico Pavignani and Allessandro Colombo:
Sustainability is continuously invoked as a key criterion to assess any aid-induced activity or initiative. Sometimes, the concept is given the weight of a decisive argument. Thus, to declare something “unsustainable” may sound as equivalent of “worthless” or even “harmful,” in this way overruling any other consideration.28
Pablo Gottret and Georges Schieber reiterate this common definition of sustainability in their observation that “[s]ustainability has generally been described in terms of self-sufficiency.”29 Both of these observations suggest that, at present, international assistance will not support any distribution of health-related goods that cannot be sustained by the country itself. In other words, international assistance will only support distribution of health-related goods efforts that the beneficiary country could sustain independently (and if it could sustain these efforts independently, the international assistance would not be necessary). It should come as no surprise, therefore, that international assistance has not made a big difference.
However, it is not entirely correct that sustainability (in the sense of self-sufficiency) is invoked as a criterion for all aid-induced activities. Certainly it is not required in humanitarian or medical relief interventions. The medical relief paradigm was originally designed to respond to acute health crises, to “help populations get back to where they were before disaster struck.” 30 Therefore, the criterion of sustainability is not really considered when determining the appropriateness of the medical relief response; as the crisis is supposed to be temporary, it is assumed that long-term response will not be necessary.
Those who practice the medical relief paradigm have faced their greatest challenges in the case of chronic health crises. These include the epidemics of HIV/AIDS, tuberculosis, and malaria, but also recurring episodes of malnutrition, and even generalized lack of access to the most basic level of health care. Alan Whiteside and Amy Whalley blame humanitarian actors for their failure to “provide clear guidelines as to when an event is severe enough to be declared an emergency” and “recognize change in the nature of disasters,” with the result that they do not address the real humanitarian crises.31
This has changed in recent years, with humanitarian organizations becoming more responsive to chronic health crises. Such organizations, however, continue to rely on expatriate implementers and parallel management systems and the need to remain independent from governments, distancing strategies designed to allow humanitarian organizations to act in acute crises and interventions in armed conflicts in particular. Such strategies seriously limit the potential of such organizations to respond to chronic health crises.
Indeed, one should not expect that the two classic international assistance for health paradigms will be adequate to successfully redress global health inequalities. One is too focused on domestic self-reliance; the other has to remain independent from the governments of the countries in which it operates. The global AIDS response began as a medical relief response out of necessity, not only because the HIV/AIDS epidemic created a crisis situation in high prevalence countries, but also because the health development paradigm could not accommodate the costs of AIDS treatment.32 Medical relief organizations like Médecins Sans Frontières (MSF) were among the first to provide AIDS treatment in low-income countries. The President’s Emergency Plan for AIDS Relief (PEPFAR) of the USA contains both “emergency” and “relief” in its name; both words attest to the medical relief roots of the global AIDS response.
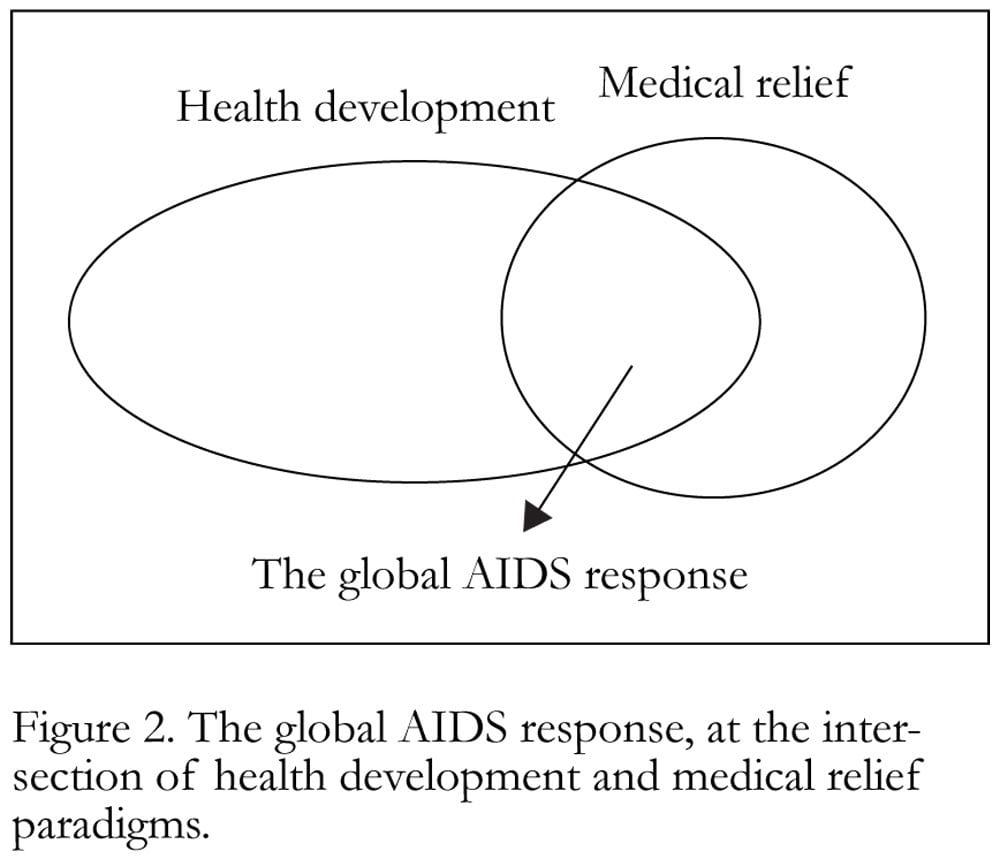
Distinguishing between operational sustainability and financial sustainability is essential to understanding how the global AIDS response evolved from its medical relief roots. Figure 2 illustrates its place at the intersection of health development and medical relief. Like health development efforts, the global AIDS response aims for operational sustainability in the conventional sense of self-sufficiency. And like medical relief efforts, it relies on sustained international financial support. Michel Kazatchkine, the executive director of the Global Fund, identified the development of this intersection in his closing speech at the XVII International AIDS Conference, noting, “The Global Fund has helped to change the development paradigm by introducing a new concept of sustainability. One that is not based solely on achieving domestic self-reliance but on sustained international support as well.”33
This new paradigm of international assistance for health — aiming for operational self-sufficiency without aiming for financial self-sufficiency — clearly has broad potential application and counters the argument that only endogenous efforts effectively reduce health inequalities. The World Health Organization (WHO)’s 2008 report acknowledges that “the steep increase in external funds directed towards health through bilateral channels or through the new generation of global financing instruments has boosted the vitality of the health sector.”34 But the report then adds immediately that “[t]hese additional funds need to be progressively re-channeled in ways that help build institutional capacity towards a longer-term goal of self-sustaining, universal coverage.”35
The new sustainability paradigm within which the Global Fund operates was born of necessity rather than theory. And while praising the Global Fund for boosting the vitality of the health sector, WHO now argues for a return to the self-sufficiency paradigm.36 To this we respond by first asserting that the success of the Global Fund gives weight to a theory of global health justice (discussed further below), and second, that the formulation of a relevant theory is necessary to provide an important theoretical foundation for practice, both the practice of the Global Fund itself and related practices to realize global health justice.
International human rights law as a compass
In the arguments above, we have affirmed Daniels’ arguments for the obligations of global health justice and have drawn on them to push our assertions beyond the immediate limits of his philosophical narrative. On the issue of using international human rights law to establish new global health justice theory, however, we disagree.
Daniels questions the usefulness of international human rights law as a compass to navigate between the dual risks of what he calls “cosmopolitan intuition” and “strongly statist versions of relational justice.” He argues that international human rights law says very little about global health justice because the obligation of progressive realization of social human rights is closely linked to the availability of national resources. His reasoning can be illustrated by comparing maternal mortality in Norway with that in Burundi.37 For example, if the risk of dying while giving birth is a hundred times higher for a woman living in Burundi than for a woman living in Norway, such risk discrepancy does not necessarily reflect a violation of the right to health. Such a violation would exist if the maternal mortality level in Burundi results from insufficient allocation of government revenue to maternal health care services, or from discrimination against part of the population. But if Burundi’s higher maternal mortality is merely the result of insufficient government revenue — the result of Burundi being a very poor country — then it would not constitute a violation of the right to health. In Daniels’ words:
Consequently, some inequalities may fall within the range of reasonable efforts at progressive realization of the right to health. In addition, because of their unequal resources, different states may achieve unequal health outcomes while still securing the right to health and health care for their populations.38
Daniels’ reasoning seems to exclude any consideration of international assistance. Surely, any evaluation of progress made in realizing the right to health globally must consider scarcity of available resources. But estimates of available resources should not be limited to government revenue; they should also include resources from international assistance.
However, including resources from international assistance is problematic in many aspects. Should one consider the quantitative value of present international assistance? Or should one consider the quantitative value of the international assistance that a country ought to receive? And if the latter is the case, then how do we ascertain how much international assistance a country like Burundi ought to receive?
To answer these questions, we suggest the concept of core content of social human rights as a useful conceptual tool. In offering this new suggestion, we are building further on an element contained in Daniels’ system. Replying to Thomas Nagel, Daniels explains his own rejection of the “strongly statist versions of relational justice” by explaining that “Nagel rejects the idea that we might work out a “sliding scale” of obligations that falls between state-mediated justice and the cosmopolitan view, that is, in the space in which I am proposing we work out our obligations.”39 We argue below that indeed the concept of core content of social human rights offers such a sliding scale, in the space between state-mediated justice and the cosmopolitan view. But before we proceed to this argument, it is first necessary to identify the key sources of international human rights law that enable us to develop such an argument. These include 1) the 1948 Universal Declaration of Human Rights (UDHR); 2) two derivative international covenants, the International Covenant on Civil and Political Rights (ICCPR) and the International Covenant on Economic, Social and Cultural Rights (ICESCR); 3) the 1989 Convention on the Rights of the Child (CRC); and 4) the Committee on Economic, Social and Cultural Rights general comment on the right to health.
While the 1948 UDHR is the foundation of international human rights law, it is not a legally binding document in itself, but expresses values later embodied in legally binding obligations through international human rights treaties that are based on it.40 The ICCPR and the ICESCR are two examples of such documents derived from the UDHR that contain legally binding obligations for the states that ratify them.41 Article 12 of the ICESCR defines the right to health as “the right to the highest attainable standard of physical and mental health,” and the related obligations include the provision of health care services and of preconditions of health, including access to safe water, food security and housing.42 This basic definition is affirmed and expanded in later international conventions, including the CRC and other national and international legislation.43 A further important development occurred in 2000 when the Committee on Economic, Social and Cultural Rights (the Committee) issued a general comment on the right to health, addressing the scope of the right to health and the importance of international cooperation in achieving the right to health.44 Whereas the language of article 2(1) of the ICESCR does not allow distinguishing between national and international obligations — countries are bound “to take steps, individually and through international assistance and co-operation” — the general comment on the right to health clarifies the scope of national and international obligations.
A key element of social rights is that they are expected to be realized in a progressive manner, over time, in accordance with available resources.45 As this relates to the right to health, the Committee notes: “The concept of progressive realization constitutes a recognition of the fact that full realization of all economic, social and cultural rights will generally not be able to be achieved in a short period of time.”46 The concept of progressive realization should never be misinterpreted to justify endless delays in realizing social rights. It is not to be viewed as “an escape hatch (for) recalcitrant states.”47 Such an interpretation would deprive social rights of any meaningful value. Thus, the Committee notes that States parties have “an obligation to move as expeditiously and effectively as possible.”48 Against any idea that “progressive realization” might imply “no immediate obligations,” the Committee emphasizes a series of concepts and principles that define the nature of States’ obligations, including the principle of non-retrogression (a state should not take steps backwards), the principle of non-discrimination, and the concept of core content. We will focus here on the concept of core content, as it is the key principle of international human rights law that gives rise to obligations of global health justice, and, as such, might be used to clarify obligations of global health justice.
The Committee defined the core content of the right to health through its definition of the core obligations that arise from the right to health. Core obligations include obligations to ensure access to essential health services and promotion of the preconditions of health. Essential health services include the provision of essential drugs, as defined by the WHO.
For most health practitioners in developing countries, this definition sounds like a wild dream. Low-income countries are simply too poor to provide a basic package of health services, which is estimated by WHO to cost US$40 per person per year.49 Given the principle of ultra posse nemo obligator, that is, the idea that no person (or country) can be obligated beyond what he, she or it is able to do, does it make sense to define core obligations that are unaffordable for low-income countries? It does, in light of article 2, para. 1 of the ICESCR, which states that “Each State Party to the present Covenant undertakes to take steps, individually and through international assistance and co-operation, especially economic and technical, to the maximum of its available resources.”50 When considering the ability or inability of low-income countries to fulfill their core obligations, that is, one should not only consider their national resources, but also resources they receive from international assistance. As Paul Hunt remarked at the May 2000 Committee session in which, the general comment on the right to health was drafted:
[I]f the Committee decided to approve the list of core obligations, it would be unfair not to insist also that richer countries fulfill their obligations relating to international cooperation under article 2, paragraph 1, of the Covenant. The two sets of obligations should be seen as two halves of a package.51
If the right to health is meaningless without the realization of at least its core content, and if some countries lack the resources needed to realize the core content of the right to health, then the right to health itself cannot exist without international obligations to provide assistance. Without international obligations to provide assistance — without global responsibility, that is — the right to health is not a right but a privilege reserved for those who are born outside of the world’s poorest countries. Such global responsibility does not mean, however, that low-income countries have an unconditional and unlimited claim to international assistance in order to realize the core content of the right to health. As Philip Alston has noted: “The correlative obligation would, of course, be confined to situations in which a developing country had demonstrated its best efforts to meet the [Millennium Development] Goals and its inability to do so because of a lack of financial resources.”52 Thus any claim to international assistance would be a conditional one, reserved for countries that demonstrate their best efforts.
We further suggest that a claim to international assistance would not only be conditional, but also limited. Article 2, para. 1 of the ICESCR — which affirms both domestic obligations and international obligations of assistance without specifying the difference between both — is confusing. If international obligations of assistance arise only when domestic obligations have been completely fulfilled, in fact they would never arise because the right to health is a moving goal and the reality is that “the highest attainable standard of physical and mental health” will never be completely attained. Under these conditional terms, high-income countries could endlessly refute international obligations of assistance, referring to their domestic obligations. The concept of core content in fact imposes a hierarchy: that it is more urgent to realize the minimum essential standard of health for all humans, without which the right to health itself becomes meaningless (or a privilege for people born in other countries than the poorest ones), than to aim for the very highest attainable standard of health domestically. This hierarchy would disappear as soon as the minimum essential standard of health were realized everywhere. At that point, in accordance with the concept of core content, rich countries could invoke the primacy of domestic obligations to argue a shift from giving international assistance to give priority instead to the highest attainable standard domestically.
Interpreting the concept of the core content of the right in this way would also provide for the possibility of a sliding scale of responsibility, one that falls between exclusively national responsibility and wholly global responsibility (more on this below). It would provide a compass to navigate between that Scylla and Charybdis that Daniels identified, that is, between the fraught risks of “cosmopolitan intuition” and “strongly statist versions of relational justice.” While we agree to a certain extent with Katharine Young’s comment, according to which ‘minimum core’ or ‘core content’ is a “concept in search of content,” we believe that our use of it here is consistent with the Committee’s general comment on the right to health, and that it does give content to the concept even if it fails to answer all of Young’s concerns.53
Taking up Daniels’ challenge: Toward a new paradigm?
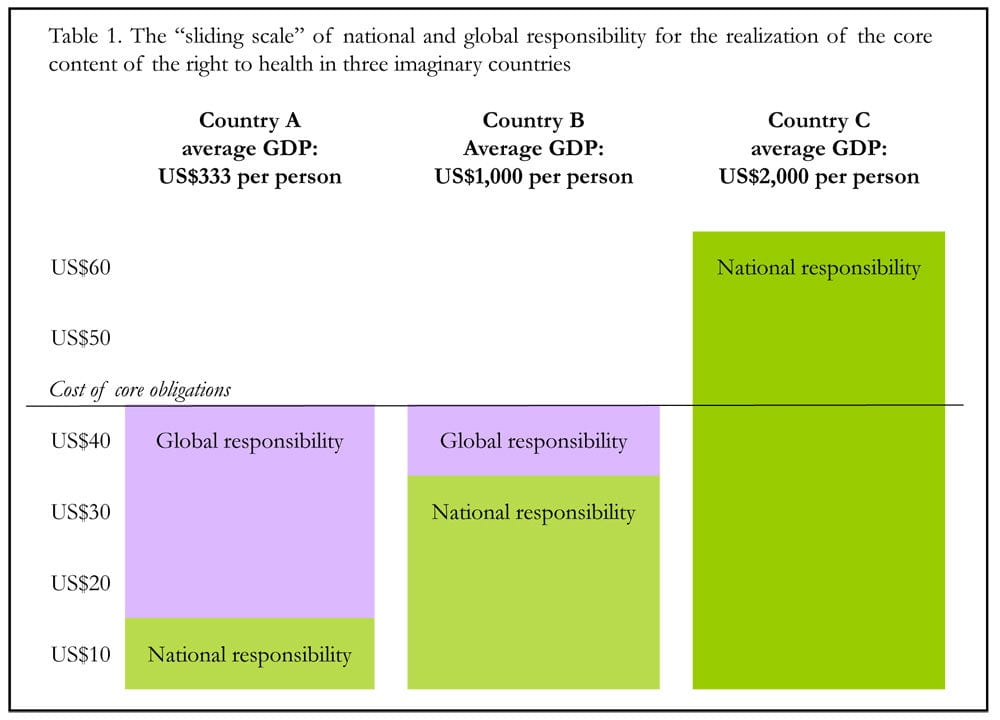
In the discussion below, illustrated by Figure 3 and Table 1, we outline the new paradigm suggested above by drawing on two separate assumptions, in addition to the 2001 pledge by African Heads of State and Government to allocate at least 15% of their budget to the health sector.54 First, we assume that, in order to realize the core content of the right to health, governments must be able to spend at least the US$40 per person per year on health-related good identified by WHO as necessary for an “adequate package of healthcare interventions” (adjusted for inflation).55 Second, we assume that government revenue, excluding grants, in low-income countries could reach 20% of GDP.56 If we then integrate the second of these two assumptions with the Abuja Declaration, we can identify a general benchmark that low-income countries should mobilize. This benchmark would require that they raise and allocate the equivalent of 3% of their GDP to the distribution of health-related goods, in order to satisfy the requirement that they are making “best efforts” to realize the core content of the right to health.
In Table 1, we illustrate how such a sliding scale would work. Country A has a GDP per person of US$333 and is assumed to be able to spend 3% of this amount, or US$10 per person per year, on the distribution of health-related goods. The global responsibility towards country A is limited to ensuring that it can achieve health-related goods distribution worth US$40 per person per year, assuming that this financing level is what it takes to realize the core content of the right to health, or the equivalent of US$30 per person per year. Country B has a GDP per person of US$1,000, and is able to spend 3% of that amount (or US$30 per person per year) on the distribution of health-related goods. The global responsibility towards country B is the equivalent of US$10 per person per year. Country C has a GDP per person of US$2,000, and is able to spend 3% of that amount (or US$60 per person per year) on the distribution of health-related goods. There is no global responsibility towards country C.
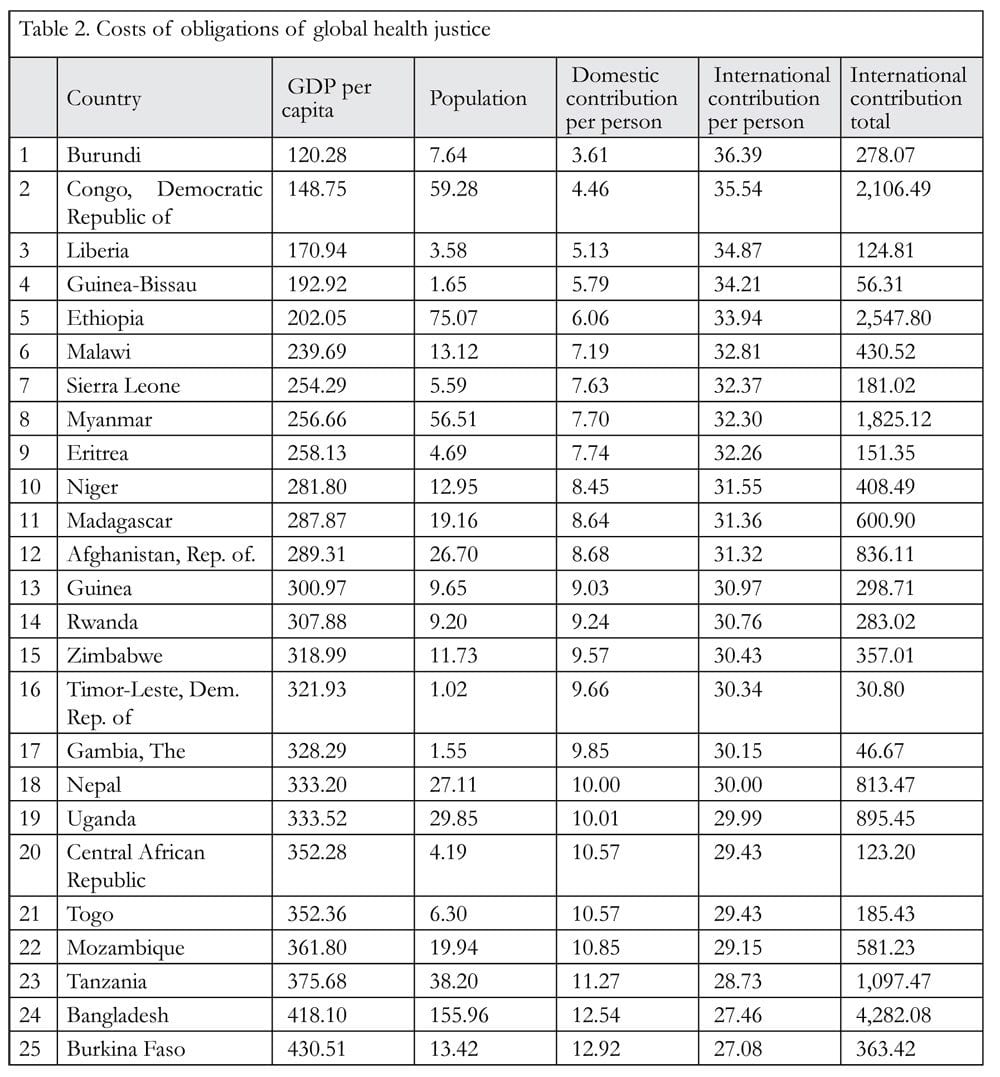
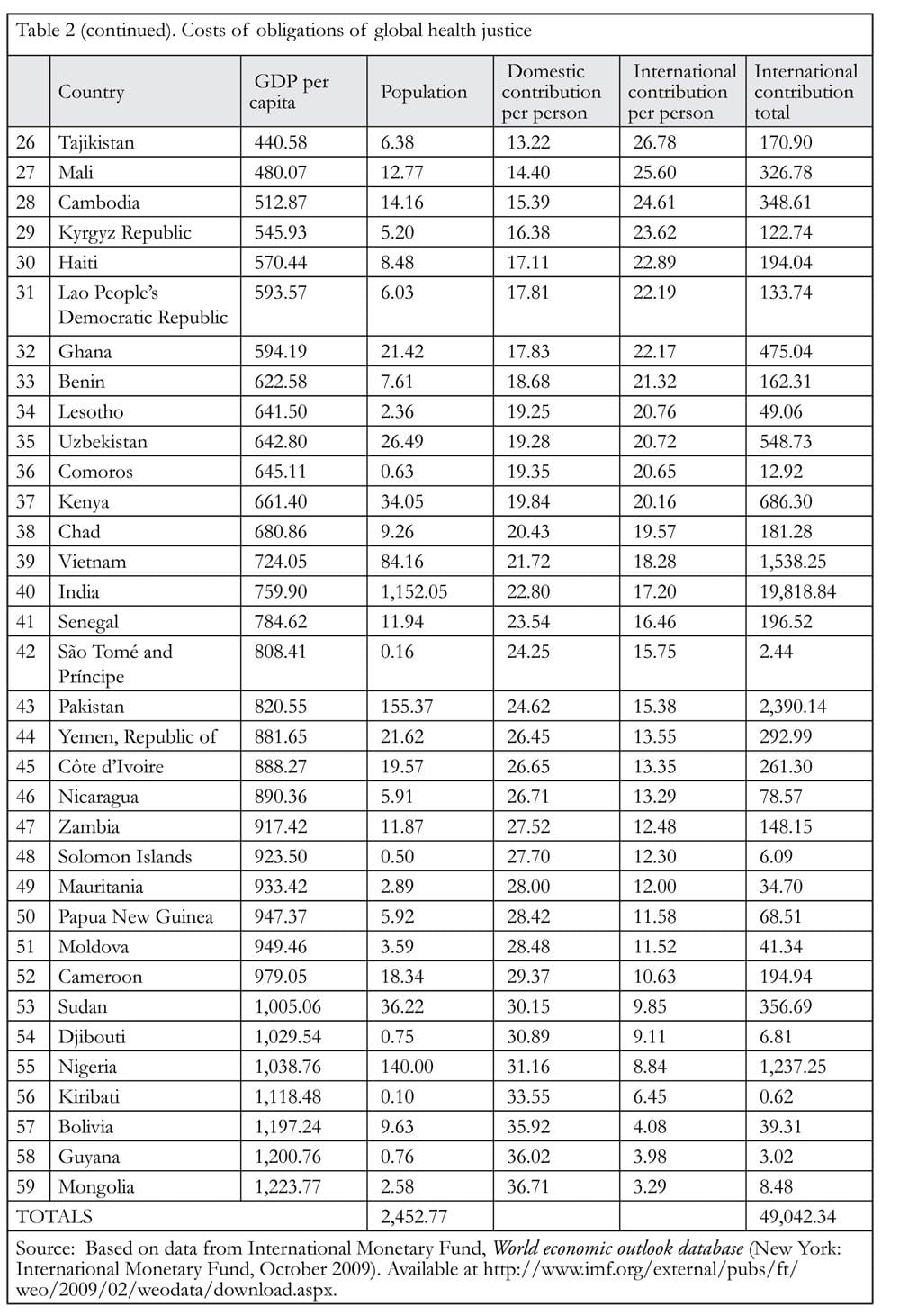
Applying such parameters as outlined above, we estimate that the cost of global responsibility for the right to health, or the cost of the obligations of global health justice, is about US$50 billion per year. This is the amount of assistance that would be needed by 59 low-income and lower-middle-income countries, representing a population of 2.5 billion. This is illustrated by Table 2 on the next page.
The 66 countries or economies presently classified as high-income by the World Bank enjoyed a collective GDP of US$43 trillion in 2008, and US$26 trillion in 2000. Even when taking into account the present global financial crisis, only an extremely pessimistic view would maintain that the collective GDP of high-income countries (and economies) will not reach US$49 trillion very soon. In other words, to live up to their global responsibility, rich countries need to allocate only about 0.1% of their GDP to international assistance for health.
In this proposed plan, which we offer in response to Daniels’ challenge, international human rights law can indeed serve in a very concrete way as a compass toward global health justice, enabling us to navigate safely between the dual risks of “cosmopolitan intuition” and “strongly statist versions of relational justice.”
Basic institutions for global health justice?
Like many philosophers thinking and writing in the tradition of John Rawls, Daniels attaches great importance to the existence of specific identifiable, basic institutions as a condition for justice. Here, too, his view differs from ours. Relationships between people can be unjust even if not governed by an identifiable institution. The identification of justice with specific institutions may suggest a confusion between situations of injustice (which do not require identifiable unjust basic institutions) and their remedies (which often do require identifiable corrective basic institutions). For example, the Matthew Effect described above, which Merton qualified as “an unintended double injustice, in which unknown scientists are unjustifiably victimized and famous ones, unjustifiably benefited,” is difficult to attribute to any identifiable and unjust basic institution.57 And yet, a basic institution might be required to counter its unjust effects. Taking his example, a corrective “institution” might perhaps take the shape of a formal and tightly enforced system of agreement between leading academic journals and/or book publishers to conduct strictly anonymous manuscript peer reviews in order to prevent publication decisions that might depend merely on authors’ reputations.
While we differ with Daniels’ emphasis on institutions as a condition for justice, he himself admits that others hold much narrower interpretations on this point. Building on the views of Joshua Cohen and Charles Sabel, Daniels writes,
Cohen and Sabel sketch three types of international relationships that might give rise to obligations of justice beyond humanitarian concerns: international agencies for distributing a specific good, cooperative schemes, and some kinds of interdependency. Each may give rise to obligations of justice, such as concerns about inclusion.58
Here we would agree with Daniels, if the global free market is understood as a global cooperative scheme, and if some of its consequences including the Matthew Effect are understood as a kind of interdependency, thus giving rise to obligations of justice. An international agency for the distribution of health-related goods is not necessary for the conclusion that the present distribution of health-related goods is unjust. We might, however, need an international agency for the distribution of health-related goods that would correct the injustice stemming from the current global system. Such a global, basic institution that might rule the distribution of health-related goods in a just manner could take several forms. It might take the form Lawrence Gostin proposed, of a Framework Convention on Global Health.59 Or it might take the form of a Global Health Fund, as we proposed elsewhere.60 In any case, some form of conventional entity is necessary in order to enforce the interactive and practical applications of national and global responsibility.
Daniels has noted that “[j]ustice may be one thing for people who stand in the relations defined by one nation-state and another for those who are members of different nation-states and interact through other kinds of institutions globally.”61 Practically speaking, for example, if Madagascar has a government revenue (excluding grants) that equal 11% of its GDP, and if its inhabitants feel that the tax burden is high enough even though their government has insufficient resources for a just distribution of health-related goods, while Ghana has a government revenue (excluding grants) equaling 24% of its GDP, how does one determine the relative roles of global responsibility for health?62 Should rich countries support Madagascar more than Ghana because the government of Madagascar has fewer resources? Or should rich countries support Ghana more than Madagascar because the inhabitants of Ghana are making a greater effort?
Likewise, what actions would support health justice in a situation where, for example, the inhabitants of Belgium, Sweden, Norway, Luxembourg, the Netherlands, and Denmark, support their respective governments in allocating the equivalent of 0.7% of their GDP or more to international assistance, while the governments of the US and Greece are allocating less than the equivalent of 0.2% of their GDP to international assistance?63 Should the inhabitants of the more generous rich countries simply accept their governments’ practice of contributing a much higher share than that of certain other rich nations?
These huge differences represent a formidable challenge inasmuch as they represent differences in opinions about global and national responsibility and about global and national health justice. However, we would argue that these situations should not be viewed as an insurmountable challenge; they require an agreement between most, if not all, countries on no more than a few parameters.
To summarize here our argument in this paper, we have demonstrated that international human rights law in general, and the concept of core content of social human rights in particular, can provide a compass to navigate between the global and national extremes of health care justice. We have noted that the primary responsibility for realizing the core content of the right to health is a national responsibility. We suggest that States should act on their global responsibility, as secondary or subsidiary responsibility for the realization of the core content of the right to health, as soon as any country exhausts its domestic resources and is still unable to realize the core content of the right to health.64 We argue that in order to fulfill global responsibilities, rich countries need not allocate more than 0.1% of their GDP to international assistance for health.
Our proposed model is in alignment with the practical recommendations of civil society groups in Europe and the US. In Europe, civil society groups with very different global health priorities (e.g. access to treatment for HIV, maternal and reproductive health) are converging around a common task, that high-income countries should allocate at least the equivalent of 0.1% of their GDP to international assistance for health.65 In the US, civil society groups are not explicitly using the 0.1% of GDP target, but they are demanding that the US contribute US$16 billion to international assistance for health, which happens to be 0.1% of the GDP of the US. 66
An agreement between most, if not all, countries on no more than a few parameters is, we suggest, all that is necessary to put this plan in place and create a basic institution for global health justice.. Such an agreement should include a consensus on how much each individual poor countries should contribute (we propose 3% of GDP), an agreement on how much they need to realize the core content of the right to health (we propose US$40 per person per year), and an agreement on how much rich countries should contribute (we propose 0.1% of GDP).
To verify the validity of these parameters, let us examine the case of Ethiopia as one example. Applying the above figures and the profile for Ethiopia listed in Table 1, Ethiopia would need US$2.5 billion per year in international assistance for health. The government of Ethiopia recently estimated the cost of its health sector plan at US$1.9 billion per year; with a population of 80 million people, this is still less than US$25 per person per year. This estimate has been validated by the WHO, World Bank, UNFPA, UNICEF, and several donor countries including Ireland and Spain, in the form of a “Joint Financial Arrangement” according to which Ethiopia would need to spend US$1.4 billion per year on health care, in addition to the US$0.5 billion it spends on health care at present.67 About 80% of this US$1.9 billion per year would need to come from international assistance for health. It is obvious that the government of Ethiopia will not be able to replace this high level of international assistance with its own government revenue within the coming decades, whether one uses the target of US$2.5 billion target or the smaller target of US$1.5 billion.
Now let us imagine that Denmark, Norway, and Sweden together are willing to fill this fiscal gap by giving US$1.5 billion per year to Ethiopia for the distribution of health-related goods. Such a decision would prompt another global health justice question: why would they be willing to do that for Ethiopia and not for the other countries needing assistance? In Denmark, Norway, and Sweden, yet another global health justice question would be: why should they contribute 0.1% of their GDP to global health while other rich countries do not?
One way to answer such questions would be to establish both a convention that details the extent of national and global responsibility, and an institution that pools and redistributes contributions (or at least monitors contributions), and to which all countries would be accountable. A Global Fund for Health, along the lines of the existing Global Fund to fight AIDS, Tuberculosis and Malaria, would provide such an institution.
The Global Fund was created in 2002 “to dramatically increase resources to fight three of the world’s most devastating diseases, and to direct those resources to areas of greatest need.”68 It is a global public/private partnership that acts as a financial enabler, not as an implementer. It pools donor funds and funds proposals based on merit not political considerations.69 The Global Fund Board issues calls for proposals; countries apply for funds through a national-level Country Coordinating Mechanism (CCM) which includes representatives from governments, multilateral and bilateral agencies, non-governmental organizations (NGOs), people living with the diseases, academic institutions, and private businesses. The proposals are reviewed by the independent Technical Review Panel, which makes recommendations to the Global Fund Board. The Global Fund Board includes representatives of donor and recipient governments, NGOs from the South and the North, the private sector and communities affected by the diseases. Once a proposal is approved, a grant is signed with a Principal Recipient, proposed by the CCM. A Local Fund Agent oversees implementation, acts as an independent auditor of expenditure and activities, and liaises with the Global Fund’s Secretariat. Attempts to formalize donor country burden sharing have not yet been successful.
The Global Fund proposal process does not conform to the conventional financial sustainability norm but expands the concept of financial sustainability beyond national resources to include those of the international community.70 This implicit commitment to sustained financing was confirmed in the 2006 United Nations General Assembly Special Session on HIV/AIDS Declaration, in which member states committed themselves “to supporting and strengthening existing financial mechanisms, including the Global Fund to Fight AIDS, Tuberculosis and Malaria, as well as relevant United Nations organizations, through the provision of funds in a sustained manner.”71
A Global Fund for Health — along the lines of the existing Global Fund but with a wider health-related goods mandate — would allow for the monitoring of contributions from all high-income countries in accordance with an agreed burden-sharing key (0.1% of GDP, for example). Such a model would also ensure that all countries in need of assistance would receive it in accordance with their needs, after verifying that they are making their “best efforts.”
Conclusion
In taking up Daniels’ challenge in this paper, we have formulated what we believe is a substantiated response that has real potential for practical application. Like Daniels, we believe that obligations of global health justice do exist, that there is a global responsibility for growing inter-country inequalities in wealth that has a direct impact on global inequalities in the distribution of health-related goods, and that it is possible to imagine ways of correcting the distribution of health-related goods “in between state-mediated justice and the cosmopolitan view.”72 Our view differs from Daniels in the strength of our assertion that international human rights law can provide a compass to guide us on the forward path of defining and negotiating between national and global responsibility for health, by using the concept of core content of the right to health. We also differ from Daniels by outlining a very explicit proposal for putting this compass to work, described above.
If obligations of global health justice have not been taken seriously until recently, it is perhaps due to a naïve belief that promoting health justice within the borders of countries (through health development) in combination with some exceptional efforts for exceptional crises (through medical relief) is sufficient. We suggest that the HIV/AIDS epidemic has made it manifestly clear that this is not the case. The global AIDS response required a new paradigm, which in our view was the first real attempt at achieving global health justice.
Yet this model lacked a strong theoretical basis and, as a result, the opportunities for building on its success are now at risk, in a climate of economic caution. This is evident in the increasing number of voices arguing that the “exceptionality” of the global AIDS response is in itself a global health injustice.73 We would agree with this argument, but we reject the solution that is often proposed in the attempt to correct the “exceptionality,” namely the solution to redirect part of the funding of the global AIDS response to the distribution of other health-related goods. In our opinion, this proposed solution results from an insufficient understanding of the aim of self-sufficiency, a concept abandoned (perhaps too exuberantly) in the global AIDS response. To adopt it retrospectively for the global AIDS response would only result in less funding for the global AIDS response, not in more funding for the distribution of other health-related goods. If, instead, the solution were to expand the new approach to sustainability, based on obligations of global health justice, the result would not require reducing global AIDS funding; it would require absolute increases in funding for health, both national and international. Considering the millions of premature human deaths that such a move could prevent every year, if only obligations of global health justice were taken seriously, we believe that it is time to end such funding ambiguities. Every human death that could have been avoided at a daily cost less than the price of a cup of coffee in rich countries is an example of the continuing human tragedy of global health injustice.
Acknowledgments
Gorik Ooms’ contribution to this paper was written during a fellowship with the Global Justice Program of the Whitney and Betty MacMillan Center for International and Area Studies at Yale, generously supported by the Institute of Tropical Medicine (Belgium), the Research Foundation (Flanders), and a Fulbright scholarship of the Council for International Exchange of Scholars (USA). The authors also thank Thomas Pogge and David Álvarez García for their useful comments, but remain entirely responsible for the viewpoints and arguments in this paper.
Gorik Ooms is a human rights lawyer, doctor in medical sciences, researcher at the Institute of Tropical Medicine in Antwerp, Belgium, and former executive director of Médecins Sans Frontières (Belgium).
Rachel Hammonds is a human rights lawyer and a researcher at the Institute of Tropical Medicine in Antwerp, Belgium.
Please address correspondence to the authors c/o Gorik Ooms, Institute of Tropical Medicine, Department of Public Health, Nationalestraat 155, 2000 Antwerpen, Belgium, email: gooms@itg.be.
References
1. N. Daniels, Just health: Meeting health needs fairly (Cambridge, UK: Cambridge University Press, 2008).
2. Ibid., p. 355.
3. G. Ooms, From the global AIDS response towards global health? (discussion paper for the Hélène De Beir Foundation and the International Civil Society Support, January 2009). Available at http://www.hdbf.org/?page_id=345&lang=en.
4. In Homer’s Odyssey, book 12, Odysseus must sail through a narrow strait with the two monsters at either side, one creating a fatal whirlpool, the other lurking by a treacherous cliff; any attempt to avoid one of the two carried the risk of moving too close to the other, with fatal consequences. The situational metaphor of being in a situation “between Scylla and Charybdis” is most commonly rendered in English as “between a rock and a hard place.”
5. Daniels (see note 1), p. 346.
6. Ibid., p. 348.
7. Ibid., p. 346.
8. Ibid., p. 101.
9. J. Arras and E. Fenton, “Bioethics and human rights: Access to health-related goods.” Hastings Center Report 39/5 (2009), pp. 27–38.
10. B. Milanovic, Worlds apart: Measuring international and global inequality (Princeton: Princeton University Press, 2005).
11. N. Nunn, “The long term effects of Africa’s slave trades,” Quarterly Journal of Economics 123 (2008), pp. 139–176.
12. J. Stiglitz, “The future of global governance,” in N. Serra and J. Stiglitz (eds), The Washington consensus reconsidered: Towards a new global governance (New York: Oxford University Press, 2008), pp. 312–313.
13. D. Kar and D. Cartwright-Smith, Illicit financial flows from developing countries, 2002–2006 (Washington, DC: Center for International Policy, 2009). Available at: http://www.gfip.org/storage/gfip/economist%20-%20final%20version%201-2-09.pdf.
14. R. Merton, “The Matthew effect in science,” Science 159 (1968), pp. 56–63.
15. From Matthew 25:29, as translated in the New Revised Standard Version.
16. G. Myrdal, Rich lands and poor: The road to world prosperity (New York: Harper and Row, 1957), p. 12.
17. Ibid., p. 26.
18. Ibid., pp. 39–40.
19. Ibid., pp. 63–64.
20. T. Pogge, “Severe poverty as a human rights violation,” in T. Pogge (ed), Freedom from poverty as a human right (New York: Oxford University Press, 2007), pp. 30–53.
21. Daniels (see note 1), p. 140.
22. Ibid., p. 101.
23. R. Archer, Duties sans frontières: Human rights and global social justice (Versoix, Switzerland: International Council on Human Rights Policy, 2003). Available at: http://www.ichrp.org/files/reports/43/108_report_en.pdf, p. 1.
24. Ibid.
25. Instead of creating a secondary redistribution to adjust the primary, some societies tried to change the primary distribution of resources, and adopted communism. These attempts appear to have created other forms of injustice.
26. Daniels (see note 1), p. 344, emphasis added.
27. There has been little progress on Millennium Development Goal 4 (reducing child mortality) and 5 (improving maternal health). In contrast, there has been progress on Millennium Development Goal 6 (combating AIDS, malaria and other diseases). It can be argued that the Global Fund to fight AIDS, Tuberculosis and Malaria is one reason for this progress. See World Bank, Global monitoring report 2008: Progress on the MDGs, September 2008 Update. Available from: http://go.worldbank.org/156R5H0OG0.
28. E. Pavignani and A. Colombo, Analysing disrupted health sectors (Geneva: World Health Organization, 2009), p. 190. Available at: http://www.who.int/hac/techguidance/tools/disrupted_sectors/adhsm.pdf.
29. P. Gottret and G. Schieber, Health financing revisited: A practitioner’s guide (Washington, DC: The World Bank, 2006). Available at: http://siteresources.worldbank.org/INTHSD/Resources/topics/Health-Financing/HFRFull.pdf.
30. P. Trench, J. Rowley, M. Diarra, et al., Beyond any drought (London: Sahel Working Group, 2007). Available at: http://www.careinternational.org.uk/download.php?id=617.
31. A. Whiteside and A. Whalley, Reviewing “emergencies” for Swaziland: Shifting the paradigm in a new era (Durban, South Africa: HEARD, 2007). Available at: http://data.unaids.org/pub/Report/2007/swaziland%20emergency%20report_final%20pdf_en.pdf.
32. According to the classification of the World Bank, the combined GDP of low-income countries in 2008, stood at US$570 billion for one billion people, or US$570 per person per year (estimates obtained from the World Development Indicators database of the World Bank, on file with authors). Being very optimistic, one could expect the governments of these countries to collect government revenue of 20% of GDP, and to allocate 15% of government revenue to health-related goods; that would make US$17 per person per year, less than half of the US$40 per person per year required according to the WHO, and surely not enough to finance AIDS treatment at a cost of minimum US$150 per person per year. On the WHO requirement of US$40 per person per year, see G. Carrin, D. Evans, and K. Xu, “Designing health financing policy towards universal coverage,” WHO Bulletin 85 (2007), p. 652. Available at: http://www.who.int/bulletin/volumes/85/9/07-046664.pdf.
33. The Global Fund, “Dr. Kazatchkine’s closing speech at the XVII International AIDS Conference in Mexico” [press release], August 11, 2008. Available at: http://www.theglobalfund.org/en/pressreleases/?pr=pr_080811.
34. W. Van Lerberghe, T. Evans, K. Rasanathan, and A. Mechbal, The World Health Report 2008: Primary health care — now more than ever (Geneva: World Health Organization, 2008), p 106. Available at: http://www.who.int/whr/2008/whr08_en.pdf.
35. Ibid.
36. Ibid.
37. Daniels compares maternal mortality in Angola with that in Norway. We compare Burundi and Norway because their levels of government health expenditure are at two opposite extremes: Burundi is the country with the lowest level of government health expenditure and Norway is the country with the highest level of government health expenditure.
38. Daniels (see note 1), p. 336.
39. Ibid., p. 350, referring to T. Nagel, “The problem of global justice,” Philosophy & Public Affairs 33 (2005), pp. 113–147.
40. Universal Declaration of Human Rights (UDHR), G.A. Res. 217A (III) (1948). Available at http://www.un.org/Overview/rights.html.
41. International Covenant on Civil and Political Rights, G.A. Res. 2200A (XXI) (1966). Available at http://www2.ohchr.org/english/law/ccpr.htm. International Covenant on Economic, Social and Cultural Rights (ICESCR), G.A. Res. 2200A (XXI). (1966). Available at http://www2.ohchr.org/english/law/cescr.htm.
42. International Covenant on Civil and Political Rights (see note 41), Art. 12.
43. Convention on the Rights of the Child (CRC), G.A. Res. 44/25 (1989). Available at http://www2.ohchr.org/english/law/crc.htm.
44. Committee on Economic, Social and Cultural Rights, General Comment No. 14, The Right to the Highest Attainable Standard of Health, UN Doc. No. E/C.12/2000/4 (2000) Available at http://www.unhchr.ch/tbs/doc.nsf/%28symbol%29/E.C.12.2000.4.En.
45. Both Article 2, para. 1 of the ICESCR and Article 24, para. 4 of the CRC recognize that the right to health, as with other economic and social rights, will be achieved progressively and not immediately.
46. Committee on Economic, Social and Cultural Rights, General Comment No. 3, The Nature of States Parties’ Obligations, UN Doc. No. E/C.12/1991/23 (1990), Art. 2, para. 1.9. Available at http://www.unhchr.ch/tbs/doc.nsf/(symbol)/CESCR+General+comment+3.En.
47. S. Leckie, “Another step towards indivisibility: Identifying the key features of violations of economic, social and cultural rights,” Human Rights Quarterly, 20/1 (1998), p. 94.
48. Committee on Economic, Social and Cultural Rights, General Comment No. 3 (see note 44).
49. Carrin et al. (see note 32).
50. Emphasis added.
51. Committee on Economic, Social and Cultural Rights, Summary Record of the 10th Meeting (2000). Available at: http://www.unhchr.ch/tbs/doc.nsf/(Symbol)/d8711da53e337f75802568d9003bc930.
52. P. Alston, “Ships passing in the night: The current state of the human rights and development debate seen through the lens of the Millennium Development Goals,” Human Rights Quarterly 27/3 (2005), pp. 755–829. Note that Alston refers to Millennium Development Goals, not to core content of socioeconomic human rights. We believe the same argument can be made for the realization of the core content of socioeconomic human rights.
53. K. Young, “The minimum core of economic and social rights: A concept in search of content,” Yale Journal of International Law 33 (2008), pp. 113–175.
54. Organisation of African Unity, Abuja Declaration on HIV/AIDS, Tuberculosis and Other Diseases, Available at: http://www.uneca.org/adf2000/abuja%20declaration.htm.
55. Carrin et al. (see note 32).
56. International Monetary Fund, World Economic Outlook Database Available at: http://www.imf.org/external/pubs/ft/weo/2009/01/weodata/index.aspx.
57. R. Merton (see note 14).
58. Daniels (see note 1), p. 351–352, commenting on J. Cohen and C. Sabel, “Extra rempublicam nulla justitia?” Philosophy & Public Affairs 34 (2006), pp. 147–175.
59. L. Gostin, “A proposal for a framework convention on global health,” Journal of International Economic Law 10 (2007), pp. 989–1008.
60. G. Ooms and R. Hammonds, “Correcting globalisation in health: Transnational entitlements versus the ethical imperative of reducing aid-dependency,” Public Health Ethics 1 (2008), pp. 154–170.
61. Daniels (see note 1), p. 348.
62. On the figure of 11% for Madagascar, see International Monetary Fund, Regional economic outlook, Sub-Saharan Africa, October 2009 (Washington DC: IMF, 2009). Available at: http://www.imf.org/external/pubs/ft/reo/2009/AFR/eng/sreo1009.pdf.
63. G. Ferrieri, Measuring official development assistance from donor countries (Paris: Organisation for Economic Co-operation and Development, 2009). Available at: http://www.oecd.org/dataoecd/41/58/43638008.pdf.
64. W. Vandenhole, “Economic, social and cultural rights in the CRC: Is there a legal obligation to cooperate internationally for development?” International Journal of Children’s Rights 17 (2009), pp. 29–62 and p. 25.
65. Making progress on global health in the Spanish, Belgian and Hungarian Presidency of the European Union: Civil society recommendations (Madrid: Grupo de Interés Español en Población, Desarrollo y Salud Reproductiva, 2009). Available at: http://www.congde.org/uploads/documentos/b22158c45f15d8a97d68fecad015f4a3.pdf.
66. The future of global health: Ingredients for a bold and effective US initiative (Report of www.theglobalhealthinitiative.org: Recommendations for the President on advancing global health, October 2009). Available at: http://www.theglobalhealthinitiative.org/documents/report.pdf.
67. Federal Ministry of Health of Ethiopia, Joint statement of the Government of Ethiopia and signatory development partners, 15 April 2009 (Addis Ababa, Ethiopia: Federal Ministry of Health, 2009). Available at: http://www.internationalhealthpartnership.net/pdf/IHP%20Update%2013/Zambia/Joint%20Statement%20of%20The%20Government%20Of%20Ethiopia%20and%20Signatory%20Development%20Partners.pdf.
68. See the Global Fund website. Available at http://www.theglobalfund.org/en/whoweare/?lang=en.
69. The Framework Document of the Global Fund to fight AIDS, Tuberculosis and Malaria (Geneva: The Global Fund). Available at http://www.theglobalfund.org/documents/TGF_Framework.pdf.
70. The Global Fund to fight AIDS, tuberculosis and malaria, Proposal Form–Round 7 (Geneva: The Global Fund, n.d.). Available at http://www.theglobalfund.org/documents/rounds/7/R7_Proposal_Form_en.doc.
71. Political Declaration on HIV/AIDS, G.A. Res. 60/262 (2006), para. 41. Available at http://data.unaids.org/pub/Report/2006/20060615_hlm_politicaldeclaration_ares60262_en.pdf.
72. Daniels (see note 1), p. 350.
73. For a critique of AIDS exceptionalism, see R. England, “Are we spending too much on HIV?” British Medical Journal 334/7589 (2007), p. 344; and H. Epstein, The invisible cure: Africa, the West, and the fight against AIDS (New York: Farrar, Straus and Giroux, 2007). For an overview of the current state of the debate, see A. Whiteside, Is AIDS exceptional? (Durban, South Africa: AIDS 2031 Programmatic Working Group, Health Economics and HIV/AIDS Research Division [HEARD], Working Paper No. 25, 2009). Available at http://www.aids2031.org/pdfs/aids%20exceptionalism_paper25.pdf.