Between the court and the clinic: Lawsuits for medicines and the right to health in Brazil
João Biehl, Joseph J. Amon, Mariana P. Socal, Adriana Petryna
Health and Human Rights 14/1
Published June 2012
Abstract
Background: The Brazilian Constitution states: “Health is the right of all persons and the duty of the State.” Yet individuals in Brazil frequently face barriers to health prevention and treatment. One response to these barriers has been a “judicialization” of the right to health, with an increasing number of patients suing the government for access to medicines.Objective/Methods: This study uses a mixed methods approach to identify trends in lawsuits for medicines in the southern state of Rio Grande do Sul (RS) and to characterize patient-plaintiffs. Electronic registries were used to determine the number of health lawsuits filed between 2002 and 2009. In-depth interviews were conducted with thirty patient-plaintiffs, and 1,080 lawsuits for medicines under review between September 1, 2008 and July 31, 2009 were analyzed to assess socio-demographic, medical, and legal characteristics of patient-plaintiffs.Results: Between 2002 and 2009, the annual number of health-related lawsuits against the state of RS increased from 1,126 to 17,025. In 2009, 72% of lawsuits sought access to medicines. In-depth interviews revealed that patients are desperate to access medicines for chronic and advanced diseases, and often turn to the courts as a last resort. Among the 1,080 lawsuits examined, patient-plaintiffs were more likely to be older than 45 years (68%), retired or unemployed (71%), and low-income (among those who reported income, 53% (n=350) earned less than the national minimum wage). Fifty-nine percent of all cases were represented by public defenders. Plaintiffs reported 1,615 diseases and requested 2.8 drugs on average (range 1-16). Sixty-five percent of the requested drugs were on government pharmaceutical distribution lists; 78% of the 254 drugs on these lists were requested. In 95% of the cases analyzed, district courts ruled in favor of plaintiffs. Among the 917 cases with a final state high court ruling, 89% were in favor of the plaintiff. In justifying their rulings, judges most frequently cited the government’s obligation under the Constitution’s provision of a right to health.Discussion: Right-to-health litigation is a widespread practice in southern Brazil. Government pharmaceutical programs are struggling to fulfill their goal of expanded access and rational use of medicines, and poor patients are leveraging public legal assistance and a receptive judiciary to hold the state accountable to their medical needs. “Judicialization” is an alternative pathway for accessing health care, increasingly understood as access to medicines of all kinds. Tracking the health outcomes and budgetary impacts of right-to-health court cases could help inform adequate treatment policy and evaluate trends in access.Introduction
Across Brazil, patients are seeking, and sometimes realizing, access to treatment through the courts, a phenomenon that has been termed the “judicialization of the right to health.”1 Though patients are suing the government for everything from baby formula to complex surgeries, a large portion of lawsuits are for access to medicines.2
The 1988 Constitution declared health as the “right of all persons and the duty of the State” and the creation of the country’s Unified Health System (SUS) extended free health coverage to all citizens.3 The term “judicialization” stems from an expansive definition of the meaning of the right to health and also, in part, from the passage of a landmark law in 1996 establishing free universal access to antiretroviral therapies for HIV-infected individuals.4 Ministry of Health policies and a 2000 ruling by the Supreme Court further advanced the right to medicines as part of the constitutional right to health.5
Yet despite these laws, policies, and rulings, patients have had an uneven experience in realizing access to treatment in SUS. As of May 2012, about 200,000 Brazilians take antiretroviral therapies paid for by the government. At the same time, many citizens still go to local public pharmacies only to find that basic medicines are out of stock or that their prescribed medicines are not included in official pharmaceutical distribution lists.6
As part of a broader process of decentralization, and in an effort to improve the administration of SUS, the federal Ministry of Health divided responsibility for pharmaceutical distribution between three levels of government.7 While the federal government retained some of its central role in financing public health, state and municipal health secretariats had to develop new structures to assess health needs and to administer federal and local funds for care delivery. Today, federal, state and municipal tiers of government are responsible for purchasing and distributing medicines according to specific pharmaceutical lists. The federal Health Ministry continues to finance high-cost medicines that, at the time of the study were called “exceptional medicines,” and are distributed by state health secretariats.8 Municipal governments are responsible for purchasing low-cost “essential medicines,” which are delivered at local public pharmacies. State governments finance and distribute “special medicines” that their populations require but that do not appear on either of the other two lists.9 In addition, the federal Health Ministry funds strategic programs for the control of certain infectious diseases such as HIV/AIDS, tuberculosis, and leprosy, as well as rare disorders such as Gaucher’s disease.10
With a population of 190 million, Brazil is one of the largest and fastest growing pharmaceutical markets in the world, spending more than US$17 billion on medicines in 2009.11 Government-purchased medicines make up a formidable market. The Health Ministry spent more than US$2.5 billion on the acquisition of drugs in 2007, accounting for 10.7% of its total health expenditures that year, and twice as much as in 2002.12 Public and private doctors increasingly prescribe—and patients demand—new and name-brand medicines, some of uncertain benefit.13 Newer medicines, however, are often only available through private purchase. Unable to pay out of pocket or to find low-cost generics at public pharmacies, patients are increasingly suing the government. In referring to their lawsuits, people often use the expression entrar na justiça, “to enter the judiciary” or “to enter justice.”
While the justiciability of the right to health is of increasing international interest, the volume of individual right-to-health lawsuits in Brazil stands out.14 In 2009, 5,536 cases appealing high court rulings related to the right to health reached the Superior Court of Justice, and about half of these cases (n=2,583) were for access to medicines. In the same year, the Federal Supreme Court heard 806 cases related to the right to health, 142 of which were for access to medicines.15 Many of the non-medicinal cases concerned access to items such as medical devices, prostheses, and special foods, as well as the availability of hospital beds and specialized facilities for pediatric or drug dependence treatment.
To secure access to medicines, patients can file a lawsuit against any tier of government. In addition to hiring a private lawyer, they may seek representation from various public legal services. The 1988 Constitution stipulated the creation of independent public institutions “to provide integral and free juridical assistance to those who prove to lack resources.”16 The Public Defender’s Office of the state of Rio Grande do Sul was established in 1991.17 There are now about 400 attorneys offering services in 144 of the state’s 164 districts.18 To use this service, citizens must earn less than three times the minimum wage.19 The Federal Attorney General’s Office may represent children under the age of 10, as well as other vulnerable and minority groups. University law clinics also serve those in need.
In 2009, the federal Health Ministry spent US$47.8 million on court-attained drugs, a significant increase from the US$20.4 million spent in 2008 and US$4.2 million spent in 2007. By comparison, federal expenditure on court-attained drugs in 2003 was just under US$59,000.20 In the past decade, Brazilian states have also seen a dramatic rise in lawsuits and costs for court-attained drugs, particularly in the country’s southeastern and southern regions.21
In the past five years, right-to-health litigation, particularly over access to medicines, has become a subject of contentious debate throughout Brazil and has attracted international attention.22 Yet there is little definitive evidence about the nature of this new medical and legal phenomenon and its impact on the health system. Governmental data collecting systems are tenuous at best, and concerted efforts to gather comprehensive data on lawsuits for access to medicines are only in their beginning stages.
In this article, we report on trends in lawsuits seeking access to medicines in the state of Rio Grande do Sul, which has one of the largest numbers of health-related lawsuits in the country. From a selection of 1,080 active lawsuits opened from 2002 through 2009 under review by the state Solicitor General’s office, we sought to characterize patient-plaintiffs, their medical needs, legal strategies, and judicial outcomes. We examined socioeconomic and medical characteristics of those suing for medicines, including the medical conditions and medicines being sought through the court. For those cases on appeal or under injunction, we examined the judicial reasoning of the courts in their initial ruling. In-depth interviews with patient-plaintiffs assisted by the Porto Alegre Public Defender’s Office provided an opportunity to better understand how the phenomenon of “judicialization”—and the expanding role of the judiciary in the definition and fulfillment of the right to health and the delivery of health care in Brazil—is understood by individuals with acute and chronic medical conditions.
Methods
This study used three distinct methodologies to assess the phenomenon of health-related lawsuits in the state of Rio Grande do Sul. First, publicly available records in the Solicitor General’s Office in the capital Porto Alegre were analyzed to assess trends in the overall number of health-related, and medicine-specific, lawsuits against the state. Second, in-depth interviews were conducted with patient-plaintiffs in the Porto Alegre Public Defender’s Office where free legal assistance is available to people classified as low-income (earning three times the national minimum wage or less). Third, a database of active lawsuits under review by the Solicitor General’s Office was developed to examine demographic and medical characteristics of patient-plaintiffs, as well as their legal claims and resulting judicial outcomes. As a first step, we collected information on the number of overall health-related and medicine-specific lawsuits that reached the state’s Solicitor General’s Office between 2002 and 2009. The number of health-related lawsuits was determined by overall cases in electronic registries kept by the Health Secretariat, and medicine-specific lawsuits were identified by searching the registry for lawsuits coded with the keyword “medicines.”
In-depth interviews were conducted with 30 individuals to assess patients’ experiences in seeking medicines via the judiciary. Patient-plaintiffs were identified at the Public Defender’s office in four time periods: August 2008; October to December 2009; August 2010; and August 2011. Public defenders asked clients if they were interested in participating in the study. Clients who expressed interest were told the purpose of the study and asked to consent to a 20-minute initial interview and a 45-minute follow-up interview, in a location of their choice outside of the Porto Alegre Public Defender’s Office. Participants were assured that they could decline to participate at any time, or decline to answer any questions, without negative consequences to their cases. Interviews were conducted in Portuguese using open-ended questions related to medical diagnosis, treatment access, judicial experience, and social and medical outcomes. Responses were recorded in writing and audio. The authors hand-coded the interview data and conducted a content analysis to identify key themes corresponding to the interview guide and emergent issues. More complete presentation of the results from in-depth interviews, as well as from key informant interviews with judges, lawyers, physicians, and health administrators, will be reported elsewhere.
A final component of the study was the development of a database of lawsuits for medicines filed against the state of Rio Grande do Sul and under review at the Solicitor General’s Office.23 The Solicitor General’s Office reviews lawsuits originating from the state capital Porto Alegre as well as cases originating outside the capital that a district court has ruled on and that are under appeal at the state’s high court. With the assistance of state prosecutors working on right-to-health litigation, we developed a data collection instrument to abstract information from active case files related to access to medicines. Prosecutors allowed us access to case files they were reviewing during September 1, 2008 and July 31, 2009. A team of eight research fellows collected data from case files. Each collection took 30 to 60 minutes and was conducted in a room adjacent to the prosecutors. Variables gathered included: geographic origin of the case, the demographics of plaintiffs, the form of legal representation, the plaintiffs’ medical diagnoses (according to International Classification of Diseases, ICD-10), the type and frequency of medications requested, the legal arguments employed, and the outcome of cases. Data was entered using Microsoft Access and regular checks were conducted for data quality and completeness. Univariate analysis was conducted by SPSS version 16 for variable frequency, distribution, and cross-tabulations.
The research was approved by the Health Secretariat and the Solicitor General’s Office of the state of Rio Grande do Sul, which established guidelines for data collection that guaranteed the anonymity of medical and legal information found in case files. The Director of the state’s Public Defender’s Office agreed to participant observations and interviews with patient-plaintiffs. The research was also reviewed and approved by the Institutional Review Board of Princeton University.
Results
Number of health-related lawsuits
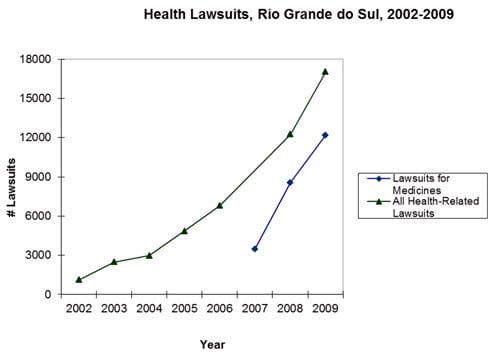
According to the official registry of the state of Rio Grande do Sul, there were 1,126 health-related lawsuits filed against the state in 2002. In 2006, 6,800 lawsuits were filed (504% increase); in 2008, 12,262 lawsuits were filed (989% increase); and in 2009, 17,025 lawsuits were filed (1,412% increase). The majority of these lawsuits—8,559 (70%) in 2008 and 12,179 (72%) in 2009—specifically requested medicines (Figure 1).
Figure 1. Number of medicine- and health-related lawsuits filed in Rio Grande do Sul, 2002-2009
Cases
In-depth interviews with patient-plaintiffs in the public defender’s office revealed how patients, suffering from chronic and advanced diseases with multiple treatment needs and unable to access medicines in state pharmacies, learn of and navigate judicial pathways to secure prescribed medicines. Patients described the importance of family support throughout lengthy and time-consuming judicial procedures. Even when they were successful in the courts, significant barriers remained to ensure ongoing and timely access to medicines for chronic health conditions. The two cases presented below were selected to illustrate the key themes outlined above.
Case 1
In 2009, Renilde sued the state of Rio Grande do Sul for medication to treat her pulmonary hypertension. The 50-year-old woman lives with her husband, a taxi driver, in a shantytown in Porto Alegre, where the couple runs an informal bar in the front portion of their brick shack. Renilde found out she was HIV-positive in 2002. She does not have trouble accessing her high-cost HIV/AIDS treatment, which she receives for free at the local health post. In early 2009, however, Renilde began feeling out of breath. Unable to perform her duties as a custodian, she lost her job. A doctor at the local health post prescribed her a medication for pulmonary hypertension. Unlike her HIV/AIDS treatment, the medicine was not offered through the public health care system at the time and cost about US$1000 a month.
Following the doctor’s advice, Renilde went to the public defender’s office. She qualified for free legal representation and sued the state for the medication. She initially lost her lawsuit but later won on appeal. A Porto Alegre district judge ordered the state to begin immediate provision of the medication, but when we interviewed Renilde in August 2009, several months had passed and she had yet to receive the drug. If she could get the medicine and improve her health, she hoped to be able to return to work and better care for her adopted teenage son.
Case 2
In August 2010, Evaldo walked into the Public Defender’s Office with his head down. His wife, Sandra, accompanied him and did most of the talking: “We cannot interrupt the treatment one more time.” Evaldo had retired as a steel factory worker and the couple, who had two adult children, resided in the nearby city of Esteio. Sandra begged the public defender to “treat us,” for “we know that people who come here get the medicine they need.”
Evaldo had chronic Hepatitis C and Sandra said that he was benefitting greatly from the 48-week treatment regimen of ribavirin and peginterferon alfa that he was receiving at the state’s public treatment center. But the doctor said that Evaldo needed 24 extra weeks of treatment, and the state’s medical expert had denied the request. The Health Ministry’s Hepatitis C treatment protocol did not allow for the extension. The doctor was able to informally guarantee Evaldo two more weeks of treatment and told him to “judicialize.”
This was the second time Evaldo had to file a lawsuit for access to his medications. In 2005, Evaldo’s public health doctor first prescribed ribavirin and peginterferon alfa. The Health Secretariat denied Evaldo’s treatment on the basis that it would constitute “re-treatment,” which the protocol does not allow. Four years earlier, in 2001, Evaldo had been treated with interferon monotherapy, which was then on the exceptional medicines list. But the supply of interferon was interrupted by the state pharmacy and Evaldo’s treatment stopped abruptly.
He won his 2005 lawsuit and said that he benefitted from the treatment, but in 2009, after developing liver cirrhosis, Evaldo’s physician recommended that he be placed on a new round of the expensive ribavirin and peginterferon alfa combined treatment regimen. Evaldo was initially able to get the medicine, but when the doctor’s request for an extension was denied, he felt desperate: “I am afraid that the legal procedure will take too long and that by the time I get the meds, if I get them, I will have to stop treatment and it will have failed once again. I need it fast.” The public defender gave Evaldo and Sandra a road map of everything they had to do, and the documents they had to bring, so that she could initiate the lawsuit the following day.
Database results
The database includes a total of 1,080 lawsuits brought against the state of Rio Grande do Sul for access to medicines. Lawsuits were opened in all years from 2002 to 2009. Nearly half of all the lawsuits (497) were initiated in 2007, and 886 (83%) were filed between 2006 and 2008. Nine hundred and forty-five lawsuits (88%) had a final district court ruling recorded and 917 (85%) had a preliminary state high court ruling. No cases had reached the Superior Court of Justice, the country’s highest appellate court, or the Federal Supreme Court, the highest court for constitutional matters.
Patient demographics
Of the 497 municipalities in the state, our database included cases that arose from 182 (37%) municipalities. Cases originating in the state capital, Porto Alegre, accounted for 20% of the sample (n=212). The majority of plaintiffs (56%, n=602) were female. Adults between 46 and 65 years of age comprised 35% (n=370) of the sample, and individuals ≥ 65 years of age comprised 32% (n=348). Forty-four percent (n=472) reported being married.
Fifty-three percent (n=459) of the 865 plaintiffs who reported their employment status were retired, 29% (n=248) were employed, and 18% (n=158) were unemployed. Among the 630 plaintiffs who reported their occupation, 40% (n=253) were retirees/pensioners; 39% (n=243) were manual laborers; 16% (n=99) were housewives; and 5.5% (n=35) were highly skilled professionals.Among the 662 plaintiffs who reported their income, 53% (n=350) earned less than the monthly national minimum wage. Sixteen individuals (1.5%) reported income equal to or greater than five times the minimum wage (Table 1).
Table 1. Characteristics of patient-plaintiffs
| N | %* | ||
| Gender | Female | 602 | 55.7 |
| Male | 478 | 44.3 | |
| Age (years) | <18 | 127 | 12.2 |
| 18-30 | 73 | 7.0 | |
| 31-45 | 125 | 12.0 | |
| 46-65 | 370 | 35.4 | |
| >65 | 348 | 33.4 | |
| Marital status | Married | 472 | 49.2 |
| Single | 307 | 32.0 | |
| Widow | 111 | 11.6 | |
| Divorced | 68 | 7.1 | |
| City | Porto Alegre | 212 | 19.6 |
| Other | 868 | 80.4 | |
| Socioeconomic status | Employed | 248 | 28.7 |
| Unemployed | 158 | 18.3 | |
| Retired | 459 | 53.1 | |
| Professional activity | Retiree or pensioner | 253 | 40.2 |
| Manual labor | 243 | 38.6 | |
| Housewives | 99 | 15.7 | |
| Professionals | 35 | 5.6 | |
| Income(Number of minimum wages) | <1 | 350 | 52.8 |
| 1-1.9 | 174 | 26.3 | |
| 2-2.9 | 67 | 10.1 | |
| 3-4.9 | 55 | 8.3 | |
| >5 | 16 | 2.4 | |
| Physician’s affiliation | Public health care system | 443 | 45.1 |
| Private practice | 362 | 36.8 | |
| University-based health clinic | 145 | 14.7 | |
| No information | 32 | 3.4 | |
| Legal representation | Public counsel | 608 | 56.3 |
| Private attorneys | 375 | 34.7 | |
| Federal Attorney General’s Office | 67 | 6.2 | |
| University law clinic | 30 | 2.8 | |
* Percentages shown refer to patients with complete information
Medical conditions
Plaintiff case files noted 1,615 different ICD-10 diagnostic codes. Twenty-one percent (n=343) were for diseases of the circulatory system; 13% (n=221) were for endocrine, nutritional, and metabolic diseases; 12% (n=199) were for mental and behavioral disorders; 9.5% (n=159) were for diseases of the nervous system; 9.4% (n=152) were for musculoskeletal system and connective tissue diseases; and 8.5% (n=142) were for diseases of the respiratory system. ICD-10 codes for diseases of the digestive system, infectious and parasitic diseases, neoplasms, diseases of the eye and adnexa, diseases of the ear and mastoid process, and diseases of the genito-urinary system amounted to less than 5% of the sample each. Neoplasms related to 16 organs and tissues were reported 67 times (4.2%). Table 2 lists the 32 ICD-10 codes most frequently cited.
Table 2. Most frequent diagnoses, according to the ICD-10 classification*
| ICD-10* | Diagnosis | N | % |
| I10 | Essential hypertension | 95 | 5.88 |
| E10 | Insulin-dependent diabetes mellitus | 90 | 5.57 |
| B18 | Chronic viral hepatitis | 62 | 3.84 |
| I25 | Ischemic heart disease | 47 | 2.91 |
| J44 | Chronic obstructive pulmonary diseases | 47 | 2.91 |
| J45 | Asthma | 46 | 2.85 |
| E78 | Disorders of lipoprotein metabolism | 42 | 2.60 |
| G20 | Parkinson’s Disease | 37 | 2.29 |
| F32 | Depressive episodes | 35 | 2.17 |
| F33 | Recurrent depressive disorder | 30 | 1.86 |
| F31 | Bipolar disorder | 29 | 1.80 |
| I20 | Angina pectoris | 29 | 1.80 |
| H40 | Glaucoma | 28 | 1.73 |
| E11 | Non-insulin-dependent diabetes mellitus | 26 | 1.61 |
| G40 | Epilepsy | 26 | 1.61 |
| I11 | Hypertensive heart disease | 22 | 1.36 |
| I50 | Congestive heart failure | 22 | 1.36 |
| G30 | Alzheimer’s disease | 21 | 1.30 |
| F20 | Schizophrenia | 20 | 1.24 |
| G35 | Multiple sclerosis | 19 | 1.18 |
| C50 | Breast cancer | 17 | 1.05 |
| J43 | Emphysema | 17 | 1.05 |
| I69 | Sequelae of cerebrovascular disease | 16 | 0.99 |
| M17 | Gonarthrosis, knee | 15 | 0.93 |
| F41 | Anxiety disorders | 14 | 0.87 |
| I64 | Stroke | 14 | 0.87 |
| N18 | Chronic renal failure | 14 | 0.87 |
| I27 | Other forms of pulmonary heart disease | 13 | 0.80 |
| M81 | Osteoporosis | 13 | 0.80 |
| E03 | Hypothyroidism | 12 | 0.74 |
| E14 | Non-specified diabetes mellitus | 12 | 0.74 |
| Z94 | Transplanted organ and tissue status | 12 | 0.74 |
| Subtotal | 942 | 58.3 | |
| Total | 1615 | 100 | |
| Average number of diagnoses per patient | 1.5 |
* International Classification of Diseases, 10th revision (ICD-10). World Health Organization, 1990 (http://www.who.int/classifications/icd/en/).
Medicines requested
On average, each of the 1,080 plaintiffs requested 2.8 drugs (range=1-16). Forty percent (n=437) requested only one drug, 22% (n=235) requested two drugs, and 24% (n=257) requested between three and five drugs. Fourteen percent (n=147) of plaintiffs requested six or more drugs. On-list drugs comprised 65% of the requests (n=1956): essential medicines 28% (n=836); exceptional medicines 27% (n=800); special medicines 11% (n=320). Four hundred and fifty-five different drugs were requested. Fifty-six percent (n= 256) of these drugs were not part of governmental pharmaceutical distribution lists. In addition to drugs, 7.5% (n=81) of plaintiffs requested other health-related items (e.g., medical devices) (n=43), medical procedures and exams (n=16), diapers (n=11), food (n=4) and hospitalizations (n=3).
Of the 983 (n=91%) plaintiffs who submitted medical prescriptions, 45.1% (n=443) were issued by a physician of the public health care system (SUS); 37% (n=362) were issued by a private practice physician; 15% (n=145) were issued by a physician from a university-based clinic; and 3.4% (n=33) had no clear physician information.
Forty-one percent (n=441) of the 1,080 lawsuits requested only drugs from governmental pharmaceutical distribution lists. Thirty-three percent (n=360) of the lawsuits requested drugs that were both on and off pharmaceutical distribution lists and 26% (n=275) of the lawsuits requested only off-list drugs. Overall, 3.5% (n=38) of lawsuits requested only essential medicines and 23% (n=251) requested only exceptional medicines.
Among the poorest plaintiffs (those who reported earning less than the monthly minimum wage), 64% (n=224) requested off-list medicines, 47% (n=166) requested exceptional medicines, 27% (n=93) requested special medicines and 40% (n=141) requested essential medicines. Among plaintiffs earning three times or more the monthly minimum wage, these figures were 58% (n=41), 52% (n=37), 13% (n=9), and 16% (n=11), respectively.
Seventy-eight percent of the 254 drugs that are part of governmental pharmaceutical distribution lists were requested at least once. All 77 drugs in the essential medicines list appeared in the lawsuits. Of the 68 drugs in the special medicines list, 39 (57%) were requested. Of the 109 drugs in the exceptional medicines list, 83 (76%) were requested. There was only one lawsuit for medicines related to a federal governmental strategic program (requesting ritonavir and tenofovir for HIV infection). Fifty-seven other drugs that are part of governmental strategic programs (n=69) were also requested, but for the treatment of conditions other than the program’s targeted diseases.
The three most requested medicines were budesonide, acetylsalicylic acid, and formoterol, which are commonly used for asthma and COPD (budesonide, formoterol) or cardiovascular disease (acetylsalicyclic acid), and included on the government’s exceptional and essential medicines list (Table 3). Table 3 lists other frequently requested drugs, their most common medical indications, availability in governmental pharmaceutical distribution lists, as well as the average market price for one month’s treatment and its comparison with the national minimum wage. The table also shows the number of additional drugs requested in the same lawsuit. The number of medicines requested varied by disease: Individuals who requested drugs to treat cardiovascular disease included, on average, a total of 6.5 drugs, while individuals who requested drugs to treat viral hepatitis included, on average, two drugs.
Table 3. Most frequently requested medicines
| Medicine | N (%) |
Government Distribution List |
Common Indication |
Price per Month (US$) |
% of Monthly Minimum Wage |
Average Number of Medicines in Lawsuit |
| Budesonide | 73(2.43) |
Exceptional |
Asthma, COPD* |
17.50 |
6.3 |
3.6 |
| Acetylsalicylic acid | 69(2.29) |
Essential |
CVD |
6.00 |
2.2 |
6.8 |
| Formoterol | 65(2.16) |
Exceptional |
Asthma, COPD* |
25.00 |
9 |
3.8 |
| Simvastatin | 65(2.16) |
Exceptional |
CVD** |
12.50 |
4.5 |
6.3 |
| Hydrochlorothiazide | 56(1.86) |
Essential |
CVD** |
3.00 |
1.1 |
6.6 |
| Omeprazole | 50(1.66) |
Essential |
Gastro esophageal reflux |
20.00 |
7.1 |
6.7 |
| Ribavirin | 46(1.53) |
Exceptional |
Hepatitis C |
100.00 |
35.7 |
2.0 |
| Peginterferon alfa | 42(1.40) |
Exceptional |
Hepatitis C |
3000.00 |
1071.4 |
1.9 |
| Atenolol | 36(1.20) |
Off list |
CVD** |
7.50 |
2.7 |
7.1 |
| Losartan potassium | 34(1.13) |
Off list |
CVD** |
30.00 |
10.7 |
6.2 |
| Furosemide | 34(1.13) |
Essential |
CVD** |
5.00 |
1.8 |
8.1 |
| Glucosamine | 34(1.13) |
Off list |
Osteo- arthritis |
60.00 |
21.4 |
3.6 |
| Clopidogrel | 33(1.10) |
Exceptional |
CVD** |
75.00 |
26.8 |
4.8 |
| Fluoxetine | 33(1.10) |
Special |
Depression |
15.00 |
5.4 |
5.1 |
| Levodopa | 33(1.10) |
Exceptional |
Parkinson |
60.00 |
21.4 |
4.5 |
| Enalapril | 32(1.06) |
Essential |
CVD** |
15.00 |
5.4 |
6.6 |
| Propatyl nitrate | 31(1.03) |
Off list |
CVD** |
10.00 |
3.6 |
7.0 |
| Insulin glargine | 31(1.03) |
Off list |
Diabetes |
150.00 |
53.6 |
1.6 |
| Tiotropium bromide | 30(1.00) |
Off list |
Asthma, COPD* |
175.00 |
62.5 |
2.7 |
| NPH insulin | 28(0.93) |
Essential |
Diabetes |
60.00 |
21.4 |
4.2 |
| Metoprolol | 26(0.86) |
Essential |
CVD** |
15.00 |
5.4 |
5.1 |
| Sertraline | 26(0.86) |
Special |
Depression |
30.00 |
10.7 |
4.3 |
| Carvedilol | 25(0.83) |
Off list |
CVD** |
15.00 |
5.4 |
5.9 |
| Amlodipine | 25(0.83) |
Essential |
CVD** |
20.00 |
7.1 |
6.7 |
| Captopril | 25(0.83) |
Essential |
CVD** |
20.00 |
7.1 |
7.8 |
| Levothyroxine | 25(0.83) |
Essential |
Hypothyroidism |
10.00 |
3.6 |
6.1 |
| Subtotal | 1007 (33.5%) | |||||
| Total | 3008 (100%) | |||||
* COPD: Chronic obstructive pulmonary disease
** CVD: Cardiovascular disease
Legal representation, defendants, and claims
Overall, 59% of the cases (n=608) were represented by public defenders, 34% (n=375) were represented by private attorneys, and 6.2% (n=67) were represented by lawyers from the federal Attorney General’s Office. Individuals who reported earning less than one minimum wage were less likely to have a private attorney than those reporting three or more times the minimum wage (25% vs. 66%, respectively).
In order to access exceptional and special medicines through the public health system, patients must show their prescriptions and file administrative requests with the Health Secretariat of Rio Grande do Sul. In 323 cases, plaintiff files showed evidence of requests for exceptional and special medicines via administrative mechanisms. In 46% (n=148) of these cases, administrative requests were granted. In the remaining cases, administrative requests were denied (14%, n=46), were still under review (8.7%, n=28), or were suspended by the Health Secretariat because the request was no longer necessary or because the patient had filed a lawsuit (21%, n=68). The outcome of the remaining cases was unknown (10%, n=33).
In 160 cases (15%), plaintiffs listed their municipality as co-defendant, and in 12 cases, (1.1%) plaintiffs listed the federal government as co-defendant. Plaintiffs’ attorneys supplied the following medical and administrative facts as the basis of lawsuits: medical need verified by a physician (92%, n=993); risk of death (53%, n=568); denial by the state of a previous administrative request for a drug that is part of governmental pharmaceutical lists (29%, n=315); medicines out of stock (11%, n=123); ineffectiveness of treatment or lack of alternative treatment (6.9%, n=75); and state’s discontinuance of treatment provision (6.8%, n=73). Two percent of plaintiffs (n=21) stated that they were unable to continue paying for treatment, and four plaintiffs (0.3%) cited the need to continue treatment they had received while on clinical trials.
Attorneys cited the following legal arguments for their clients’ lawsuits: constitutional right to health (92%, n=996); constitutional right to life (82%, n=881); constitutional principle of equality under law (16%, n=177); constitutional principle of human dignity (16%, n=175); state’s responsibility according to the principle of unity of spheres of government (13%, n=135).
In 98% of the lawsuits (n=1,062), a temporary court injunction was sought upon filing to provide immediate access to the medicines requested until a decision on the case was reached. As a part of their initial request for the provision of medicines, plaintiffs’ attorneys also sought fines (44% of the time, n=475) and liens (47%, n=508) against the state budget in order to enforce the judge’s temporary injunction and final ruling. Ninety-two percent of plaintiffs’ attorneys (n= 990) requested that the state pay for the plaintiff’s legal fees.
Outcomes of cases
In 93% (n=1,004) of all cases, district judges granted plaintiffs an immediate injunction, in full, for access to medicines; in 1.6% (n=17) of cases, they granted a partial injunction. District judges granted injunctions in 86% of cases when plaintiffs did not submit medical prescriptions (n=65, 6.0% of all cases). In 65 percent (n=42) of the cases where no prescription was present, judges requested an independent clinical evaluation of the patient.
Fines and liens were awarded by district judges as a means to enforce the state’s compliance with the injunctions and final rulings. Fines were granted in 18% (n=87) and liens were granted in 65% (n=332) of the cases when they were requested.
Ninety-two percent (n=990) of the plaintiffs in the reviewed lawsuits requested exemption of legal fees. This request was awarded by district judges in 91% (n=896) of the requesting cases. District judges cited the municipality as a co-defendant in 60% (n=96) of the 160 lawsuits that alleged municipal co-responsibility. Judges cited the federal government as co-defendant in 33% (n=4) of the 12 lawsuits that alleged federal government’s co-responsibility.
Of the 945 cases that had a record of a final district court ruling, 93% received full and 3% received partial provision of drugs (the same frequency as with the initial injunctions granted). In 122 cases, the cost of medicines exceeded the state’s threshold for automatic review by the state high court.
Among the 917 cases that had reached a state high court ruling, 815 (89%) were in favor of the plaintiff (either partial or full provision of drugs). In cases where the initial ruling was in favor of the provision of medicines, the state high court upheld the decision 90% (n=785) of the time. When initial rulings denied the provision of drugs, the state high court overturned the decision in 83% (n=30) of cases.
Judicial rationale
In district court rulings in favor of patients’ claims for drugs, judges most frequently cited core constitutional principles. Among the reasons noted in the 909 cases with complete information, Brazil’s constitutional right to health was cited 88% (n=801) of the time, and the obligation of the state government to act consistently and in solidarity with all levels of government was cited 39% (n=353) of the time. District judges also cited medical and procedural rationales such as: the patient had proper medical documentation of need (40%, n=367) and had acted in accordance with proper procedures for accessing medicines (9%, n=86); the state had not shown financial hardship (8%, n=76) or the drug requested could not be denied based on claim of lack of effectiveness (2%, n=16).
In deciding against the provision of drugs (n=36), district judges most frequently argued that the municipal or the federal government, rather than the state, was responsible (72%, n=26). In 16 cases (44%), district judges ruled that the claim was not in accordance with therapeutic guidelines issued by the Ministry of Health, and in 14 cases (39%) judges ruled that the claim had insufficient medical evidence. In 11 cases (31%), judges cited lack of evidence of drug effectiveness. Other reasons judges cited in ruling against plaintiff requests for medicines included: failure to procure the treatment via proper administrative procedures before opening the lawsuit (n=10); state budget limitation (n=9); and requests for brand-name drugs when a generic medicine was available (n=9).
The rationales cited by state high court judges when supporting or denying the provision of medicines were similar to the rationales cited by district judges (data not shown).
Discussion
Over the past decades, the executive, legislature, and judicial branches of the Brazilian government have struggled to define the meaning and scope of the right to health, with pressure from civil society through broad social mobilization (for example, demanding access to HIV/AIDS treatment) and lobbying (for example, by pharmaceutical companies seeking expanded markets). More recently, dissatisfied with the performance of the Unified Health System, a growing number of patients are filing lawsuits seeking access to medicines as a part of a constitutional guarantee of the right to health.
Despite the growing scale of lawsuits for access to medicines, and amid sharp debate about the phenomenon, there is scant information concerning the content of lawsuits and the characteristics of patient-litigants. Research into right-to-health litigation has been constrained by small samples, limited geographic coverage, and the relatively few variables examined.24 Most studies (with the exception of Pepe et al.) tend to corroborate the arguments of health policymakers and administrators that the judiciary is overstepping its role and that judicialization generates enormous administrative and fiscal burdens and widens inequalities in health care delivery.25,26 Previous research has also suggested that right-to-treatment litigation is a practice of the financially better off, and that low-income patients tend to sue for low-cost drugs while higher income patients tend to sue for very expensive drugs.27
Our research confirmed the explosive growth of lawsuits seeking access to medicines in the southern Brazilian state of Rio Grande do Sul, with over 12,000 cases in 2009 alone. This staggering number of lawsuits is unquestionably generating significant legal and administrative costs. With a population of about 11 million, the state of Rio Grande do Sul spent $30.2 million on court-mandated drugs in 2008. This expense represents 22% of the total amount spent by the state on medicines that year.28
However, our database of 1,080 lawsuits, primarily at the state high court level, and in-depth interviews with patient-plaintiffs, provides a new and nuanced view of the socio-economic and medical characteristics of those suing for medicines, and of the judicial reasoning of the courts that are overwhelming ruling in favor of patients. We found that patients are mainly low-income individuals who are not working (either because they are retired or unemployed) and who depend on the public system for obtaining both health care and legal representation. They are suing for a broad range of medicines to treat a diverse constellation of pathologies. Judges at district and higher court levels almost universally granted access to all medicines requested, recognizing the provision of medicines as an integral part of a virtually unrestricted constitutional right to health.
Renilde, the 50-year-old woman from our case study (Case 1), is unemployed and suffers from HIV and pulmonary hypertension. In many respects—her age, gender, low income, co-morbidities, and ill health—Renilde represents a typical patient in our database, and her representation by a public defender was also typical. The Public Defender’s Office has a strong presence both in the capital and in the interior, and public defenders represented the majority of cases in our study. In other aspects, Renilde was unusual. The majority of patients requested medicines that were on governmental pharmaceutical lists, and about a third of the cases, like Renilde’s, requested high-cost medicines that were off-lists and only available for private purchase. We found that few patients lost when they first sued the state.
In our database of lawsuits, of the plaintiffs who reported their employment status, more than half were retired and about one-fifth were unemployed. Among those who reported income, over half earned less than the monthly national minimum wage and relied on the free legal services of public defenders. Poor patients requested not only lower-cost essential medicines but also high-cost, exceptional, and off-list medicines—the latter two as frequently as patients with a higher income. This suggests that, despite problems in the SUS system, poor patients are to some extent able to access new diagnostics to address their complex treatment needs. Poor patients are not waiting for new and high cost medical technologies to “trickle down.”29 They are leveraging public legal assistance and a receptive judiciary to gain full access to all medicines now.30
Several limitations to our results should be considered. Cases were included in our database through a convenience sample of active lawsuits in the State Solicitor General’s Office, and represent primarily cases at the state high court level after having been referred from a district court (on appeal or automatically because of the cost of the judgment). The number and characteristics of lawsuits settled at the district court level is uncertain, as is the difference between cases appealed to the state high court and those that are not. State high court cases may be more likely to include requests for expensive or off-list medicines, but given the significant delay in hearing cases at the state high court, cases may also be biased towards patients with less advanced disease and those more aggressive in pursuing their litigation. These biases would reinforce our findings that the majority of patient-plaintiffs are older and suing for low-cost and on-list medicines as well as high-cost, off-list medicines.
Another potential limitation in our database was incomplete information of some variables. Forty-two percent of the cases included in the database lacked a description of profession, almost 20% lacked information on employment status, and 38% lacked income data. Of those who reported their income, 89% reported earning less than three times the minimum wage. The omission, or understatement, of socioeconomic data may have been a strategy among plaintiffs to demonstrate need and make the case for the incapacity to purchase medicines. While one-third of the cases in our database were represented by private attorneys, this does not necessarily imply higher socioeconomic status. In line with a 1950 federal law, 94% of plaintiffs represented by private lawyers requested that the state pay their legal fees, and judges granted 98% of those requests.
Despite these limitations, the broad range of medical diagnoses (n=1615) of individuals seeking medicines, and the number of different medicines requested (n=455), is striking. Two-thirds of the drugs requested by plaintiffs in our study were on governmental pharmaceutical distribution lists. Only about one-quarter of lawsuits were exclusively for access to high-cost exceptional medicines. Off-list drugs requested by plaintiffs were often low-cost and many had been available in the market for a long time and may have been prescribed because of adverse effects to equivalent on-list treatments (e.g., atenolol and propatylnitrate). The majority of medicines on each of the three government-level pharmaceutical lists were requested in plaintiffs’ lawsuits.
These results suggest significant problems in the government’s pharmaceutical distribution system at all administrative levels, particularly in regard to the delivery of listed medicines and to the updating of existing pharmaceutical lists. Patients are also demanding access to all medicines as a right. According to our data, judicialization of the right to health is not being driven by demands for new, expensive, and often experimental off-list drugs, but for every type of medicine imaginable. Some patient-plaintiffs may be suing for on-list medicines for uses that do not conform to public treatment protocols, such as in Evaldo’s case (Case 2). Other patients may be seeking medicines (e.g., psychiatric medicines) for off-label uses. Physicians may be prescribing name-brand medicines instead of generics listed on government distributions lists, or encouraging off-label uses of pharmaceuticals despite lack of evidence of effectiveness.
Patients in our sample were, for the most part, chronically ill. They had various co-morbidities and procured multiple drugs for their treatments. Some patients however had a single disease and demanded one high cost treatment. Hepatitis C patients like Evaldo (Case 2) made up a significant number of cases. These patients typically demanded ribavirin and peginterferon alfa, both of which are on the federal government’s exceptional medicines list. The high frequency of requests for drugs to treat chronic hepatitis C in our sample stands in sharp contrast with the rare request—one single case—for medicines for HIV/AIDS. Both pathologies have a similar prevalence in the south of Brazil and both treatments are distributed by governmental programs at no cost.31
This sharp contrast may reflect variations in the efficiency of governmental pharmaceutical distribution programs. While HIV/AIDS therapies are centrally managed and funded by the federal Health Ministry, the exceptional medicines program is decentralized and vulnerable to the vagaries of regional health policy and management. Moreover, while HIV/AIDS treatment is well established and broadly effective, hepatitis C treatment protocols are evolving and treatment effectiveness can be uncertain. Lawsuits may be a mechanism with which to challenge hepatitis C treatment protocols that limit access. Rather than accepting these protocols, our results show that judges give broad deference to individual circumstances and physicians’ prescriptions, deference that may undercut efforts to rationalize pharmaceutical use.32
Our results found that while the government has advanced a system of decentralized responsibility for different medicines at specific administrative levels—municipal, state, federal—plaintiffs tend to hold states responsible for all types of medicines, and judges rarely disagree. While state attorneys frequently argue that the state is not responsible for the provision of certain services, judges cite the principle of “solidarity” between levels of government to assert broad responsibility.33 Yet, while nearly all patient-plaintiffs in our study were awarded access to medicines by the court, the percentage of patients who in fact received them, or received them consistently, is unknown.
Conclusion
Our study shows that right-to-health litigation is a widespread practice, accessible even to very poor individuals. A growing number of citizens are acting within the state to guarantee their right to health. This judicialization has emerged in the context of a progressive but ailing SUS and has become a last resort or an alternative pathway for accessing health care, increasingly understood as access to medicines. Widespread and often desperate patient demand, informed by physicians’ prescriptions and facilitated by public defenders, drives the phenomenon of judicialization, and an expansive reading of the constitutional right to health on the part of judges sustains it.
Our interviews with patient-plaintiffs suggest that judicialization is now part of the medical lexicon. Physicians routinely introduce patients to the possibility of judicializing and encourage them to pursue it in order to access prescribed medicines. Further studies could help tease out the relationship between this novel court-clinic interface and the pharmaceutical business strategies in Brazil. The role of pharmaceutical companies in supporting specific patient associations and providing private judicial assistance for access to high-cost treatments not yet included in the official pharmaceutical lists should be explored. Judicialization has indeed become a parallel infrastructure in which patient-citizens and various public and private health actors and sectors come into contact, face off, and enact one-by-one rescue missions. Meanwhile, systemic challenges related to health financing, care delivery, and the social determinants of health remain under-explored.
As a “right to medicines” is consolidated in Brazil, the various branches of government have yet to develop a systematic approach to tackling drug costs and financing, as well as to determine the responsibilities of private health insurance plans in covering drug costs (which they currently do not). Attention is also needed to broader aspects of the right to health, including structural-rights interventions and social determinants of health such as education, water, sanitation, vector control, air pollution, and violence prevention.34 These complementary rights are critical to addressing the health needs of vulnerable, chronically ill, and co-morbid individuals in our database and the Brazilian population overall.
In April 2009, the Brazilian Supreme Court held a rare public hearing to examine the pressing challenges posed by right-to-health litigation.35 As an immediate outcome, a long overdue updating of government pharmaceutical distribution lists took place. The Brazilian National Council of Justice also issued a set of recommendations for judges, urging them to attend to scientific evidence and to strive for “more efficiency” when ruling in health-related cases. Even as judges recognize the constitutionality of individual lawsuits and grant requested medicines in the overwhelming majority of cases, the Brazilian judiciary has avoided directly requesting changes in policy or issuing decisions that would affect the public health system more broadly.
Rather than merely responding to individual cases, the judiciary should foster health as a collective right and pursue strategies to ensure universal availability of medicines that the government has a legal responsibility to provide. Local governments should track court cases and use them to inform efforts to remedy administrative shortcomings and public health budgetary planning. Civil society, currently engaged in seeking medicines, should also press governments to improve public health infrastructures and to address health and human rights broadly. Until more fundamental changes are realized, Brazil should ensure the adequate delivery of essential medicines and increase the transparency and efficiency with which medicines are evaluated for inclusion in pharmaceutical lists and provided to those with demonstrated need.
Funding
Research funding was provided by the Ford Foundation, Princeton University’s Health Grand Challenges Initiative, and the Woodrow Wilson School of Public and International Affairs.
Acknowledgements
The development of the research benefited from an institutional collaboration between Princeton University, Human Rights Watch, the Secretaria Estadual da Saúde do Estado do Rio Grande do Sul, and the Procuradoria Geral do Estado do Rio Grande do Sul. We acknowledge the support of Princeton University’s Center for Health and Wellbeing, Defensoria Pública do Estado do Rio Grande do Sul, Núcleo de Pesquisa em Medicamentos and Fundação Médica do Rio Grande do Sul of the Hospital de Clínicas de Porto Alegre. The analysis and interpretation expressed in the article are those of the co-authors and do not necessarily reflect those of the institutions acknowledged above. We appreciate the assistance of Alex Gertner and the comments of the two anonymous peer reviewers of the article.
João Biehl is Susan Dod Brown Professor of Anthropology and Woodrow Wilson School Faculty Associate at Princeton University in Princeton, NJ, USA.
Joseph J. Amon is Director of the Health and Human Rights Division of Human Rights Watch in New York, NY, USA.
Mariana P. Socal is a Doctoral Student in Health Systems at the Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Adriana Petryna is Edmund J. and Louise W. Kahn Term Professor in Anthropology at the University of Pennsylvania in Philadelphia, PA, USA.
Please address correspondence to the authors at jbiehl@princeton.edu.
References
1. J. Biehl, A. Petryna, A. Gertner, J.J. Amon, and P.D. Picon, “Judicialisation of the right to health in Brazil,” Lancet 78/2 (2011), pp. 2182-2184; O. L. M. Ferraz, “The right to health in the courts of Brazil: Worsening health inequities?” Health and Human Rights: An International Journal 11/2 (2009), pp. 33-45; V. L. M. Pepe, M. Ventura, J. M. B. Sant’ana, T.A. Figueiredo, V.R. de Souza, L. Simas, and C.G.S. Osorio-de-Castro, “Caracterização de demandas judiciais de fornecimento de medicamentos ‘essenciais’ no Estado do Rio de Janeiro, Brasil,” Cadernos de Saúde Pública 26/3 (2010), pp. 461-471.
2. C. Colucci, “Triplicam as ações judiciais para obter medicamentos,” Folha de São Paulo (September 9, 2009). Available at http://www.sindifarmajp.com.br/noticias.php?not_id=765; M. Scheffer, A.L. Salazar, and K.B. Grou, O remédio via justiça: um estudo sobre o acesso a novos medicamentos e exames em HIV/Aids no Brasil por meio de ações judiciais (Brasília, DF: Ministério da Saúde, 2005).
3. Constituição Federal do Brasil, Art. 196: Da Saúde (1988). Available at http://dtr2004.saude.gov.br/susdeaz/legislacao/arquivo/01_Constituicao.pdf; J. Paim, C. Almeida, L. Bahia, and J. Macinko, “The Brazilian health system: History, advances, and challenges,” Lancet 26/3 (2010), pp. 461-471; S.M. Porto, M.A.D. Ugá, and R.S. Moreira, “Uma análise da utilização de serviços de saúde por sistema de financiamento: Brasil 1998-2008,” Ciência & Saúde Coletiva 16/9 (2011) , pp. 3795-3806.
4. J. Biehl, Will to live: AIDS therapies and the politics of survival (Princeton, NJ: Princeton University Press, 2007).
5. Acórdão. RE 271286 AgR/RS. Agravo Regimental no Recurso Extraordinário. Relator: Celso de Mello (Supremo Tribunal Federal, Diário da Justiça Eletrônico, RE 271286 AgR/RS, November 24, 2000). Available at http://www.stf.jus.br/portal/diarioJustica/verDiarioProcesso.asp?numDj=226&dataPublicacaoDj=24/11/2000&incidente=3542020&codCapitulo=5&numMateria=37&codMateria=3.
6. S. Mendis, K. Fukino, A. Cameron, R. Laing, A. Filipe Jr., O. Khatib, J. Leowski, and M. Ewene, “The availability and affordability of selected essential medicines for chronic diseases in six low- and middle-income countries,” Bulletin of the World Health Organization 85/4 (2007), pp. 279-288.
7. Ministério da Saúde, Da excepcionalidade às linhas de cuidado: o Componente Especializado da Assistência Farmacêutica. Série B. Textos Básicos de Saúde (Brasília, DF: Ministério da Saúde, 2010).
8. In 2009, the federal Health Ministry changed the name “exceptional medicines” to “specialized medicines.” Available at http://www.cidades.gov.br/ministerio-das-cidades/legislacao/portarias/portarias-2009/Binder1.pdf/view.
9. Ministério da Saúde, Política nacional de medicamentos (Brasília, DF: Ministério da Saúde, 2001).
10. Ministério da Saúde, Programas estratégicos (Brasília, DF: Ministério da Saúde, n.d.).
11. Sindicato da Indústria de Produtos Farmacêuticos, Indicadores econômicos. Vendas em Reais (R$). Available at http://www.sindusfarmacomunica.org.br/indicadores-economicos.
12. F.S. Vieira, “Ministry of Health’s spending on drugs: Program trends from 2002 to 2007,” Revista de Saúde Pública 43/4 (2009), pp. 674-681.
13. A. Petryna, When experiments travel: Clinical trials and the global search for human subjects (Princeton, NJ: Princeton University Press, 2009); M.V. Souza, B.C. Krug, P.D. Picon, and I.V.D. Schwartz, “Medicamentos de alto custo para doenças raras no Brasil: o exemplo das doenças lisossômicas,” Ciência & Saúde 15/Supl. 3 (2007), pp. 3443-3454; A. Gertner, “Science of uncertainty: Making cases for drug incorporation in Brazil,” Anthropological Quarterly 83/1 (2010), pp. 97-122.
14. J.J. Amon and T. Kasambala, “Structural barriers and human rights related to HIV prevention and treatment in Zimbabwe,” Global Public Health 4/6 (2009), pp. 528-545; V. Guari and D.M. Brinks, (eds), Courting social justice: Judicial enforcement of social and economic rights in the developing world (Cambridge: Cambridge University Press, 2008), H.V. Hogerzeil, M. Samson, J.V. Casanovas, and L. Rahmani-Ocora, “Is access to essential medicines as part of the fulfillment of the right to health enforceable through the courts?” Lancet 368/9532 (2006), pp. 305-311; A.E. Yamin and O. Parra-Vera, “Judicial protection of the right to health in Colombia: from social demands to individual claims to public debates,” Hastings International and Comparative Law Review 33/2 (2010), pp. 101-130.
15. I.W. Sarlet, “Access to medicines and the judiciary: Some remarks in the light of the Brazilian experience” (presentation at The Judiciary and the Right to Health: An International Conference, Princeton University, Princeton, NJ, March 25-26, 2010).
16. Constituição Federal do Brasil, Art. 5 (1988). Available at http://dtr2004.saude.gov.br/susdeaz/legislacao/arquivo/01_Constituicao.pdf.
17. F.L.M. Souza, A defensoria pública e o acesso à justiça penal (Porto Alegre: Nuria Fabris, 2011).
18. Jus Brasil, Defensoria pública prevê atender todo Estado ainda este ano (2012). Available at http://dp-rs.jus-brasil.com.br/noticias/3032606/defensoria-publica-preve-atender-todo-estado-ainda-este-ano.
19. At the time of the study the national monthly minimum wage was about US$280.
20. Colucci (see note 2).
21. D. Diniz, M. Medeiros, and I.V.D. Schwartz, “Consequências da judicialização das políticas de saúde: custos de medicamentos para as mucopolissacaridoses,” Cadernos de Saúde Pública 28/3 (2012), pp. 479-489; S.B. Marques and S.G. Dallari, “Garantia do direito social à assistência farmacêutica no Estado de São Paulo,” Revista de Saúde Pública 41/1 (2007), pp. 101-107.
22. S. Azevedo, “Remédios nos tribunais,” Revista Época (December 12, 2007). http://revistaepoca.globo.com/Revista/Epoca/0,,ERT59499-15257,00.html; “An injection of reality,” The Economist (Editorial, July 30, 2011). Available at http://www.economist.com/node/21524879.
23. See “Projeto de criação da primeira coorte brasileira de acesso judicial a medicamentos no Rio Grande do Sul.” Available at http://www.princeton.edu/grandchallenges/health/research-highlights/aids/Database-project.pdf.
24. D.C.L. Borges and M.A.D. Ugá, “Conflitos e impasses da judicialização na obtenção de medicamentos: as decisões de 1a instância nas ações individuais contra o Estado do Rio de Janeiro, Brasil, em 2005,” Cadernos de Saúde Pública 26/1 (2010), pp 59-69; A.L. Chieffi and R.B. Barata, “Judicialização da política pública de assistência farmacêutica e eqüidade,” Cadernos de Saúde Pública 25/8, (2009), pp. 1839-1849; Marques and Dallari (see note 19); A.M. Messeder, C.G.S. Osório-de-Castro, and V.L. Luiza, “Mandados judiciais como ferramenta para garantia do acesso a medicamentos no setor público: A experiência do Estado do Rio de Janeiro, Brasil,” Cadernos de Saúde Pública 21/2 (2005), pp. 525-534; F.S. Vieira and P. Zucchi, “Distorções causadas pelas ações judiciais à política de medicamentos no Brasil,” Revista de Saúde Pública 41/2 (2007) pp. 1-8; J. Pereira, R. Santos, J. Nascimento Jr., and E. Schenkel, “Situation of lawsuits concerning the access to medical products by the Health Department of Santa Catarina State, Brazil, during the years 2003 and 2004,” Ciência & Saúde Coletiva 15/Supl. 3 (2007), pp. 3551-3560
25. Pepe et al. (see note 1)
26. Ferraz (see note 1).
27. V.A. Da Silva and F.V. Terrazas, “Claiming the right to health in Brazilian courts: The exclusion of the already excluded,” The Social Sciences Research Network (SSRN), 2008. Available at http://ssrn.com/abstract=1133620; Chieffi and Barata (see note 24); Vieira and Zucchi (see note 24).
28. Biehl et al. (see note 1).
29. D. Cutler, D. Angus and A. Lleras-Muney, “The determinants of mortality,” Journal of Economic Perspectives 20/3 (2006), pp. 97-120.
30. J. Biehl and A. Petryna, “Bodies of rights and therapeutic markets,” Social Research 78/2 (2011), pp. 359-386.
31. C.T. Cerreira and T.R. Silveira, “Hepatites virais: aspectos da epidemiologia e da prevenção,” Revista Brasileira de Epidemiologia 7/4 (2004), pp. 473-487; Ministério da Saúde, Boletim epidemiológico AIDS & DST (ano VI n°01) (Brasília, DF: Ministério da Saúde, 2009).
32. P.D. Picon and A. Beltrame (eds), Protocolos clínicos e diretrizes terapêuticas (Brasília, DF: Ministério da Saúde, 2002).
33. I.W. Sarlet and L. Timm (eds), Direitos fundamentais, orçamento e reserva do possível, 2nd ed., (Porto Alegre, RS: Livraria do Advogado Editora).
34. C.G. Victora, M.L. Barreto, C.A. Monteiro et al., “Health conditions and health-policy innovations in Brazil: The way forward,” Lancet 377/9779 (2011), pp. 2042-2053.
35. http://www.stf.jus.br/portal/cms/verTexto.asp?servico=processoAudienciaPublicaSaude