Mental health and inequity: A human rights approach to inequality, discrimination, and mental disability
Jonathan Kenneth Burns
Health and Human Rights 11/2
Published December 2009
Abstract
Mental disability and mental health care have been neglected in the discourse around health, human rights, and equality. This is perplexing as mental disabilities are pervasive, affecting approximately 8% of the world’s population. Furthermore, the experience of persons with mental disability is one characterized by multiple interlinked levels of inequality and discrimination within society. Efforts directed toward achieving formal equality should not stand alone without similar efforts to achieve substantive equality for persons with mental disabilities. Structural factors such as poverty, inequality, homelessness, and discrimination contribute to risk for mental disability and impact negatively on the course and outcome of such disabilities. A human rights approach to mental disability means affirming the full personhood of those with mental disabilities by respecting their inherent dignity, their individual autonomy and independence, and their freedom to make their own choices. A rights-based approach requires us to examine and transform the language, terminology, and models of mental disability that have previously prevailed, especially within health discourse. Such an approach also requires us to examine the multiple ways in which inequality and discrimination characterize the lives of persons with mental disabilities and to formulate a response based on a human rights framework. In this article, I examine issues of terminology, models of understanding mental disability, and the implications of international treaties such as the United Nations Convention on the Rights of Persons with Disabilities for our response to the inequalities and discrimination that exist within society — both within and outside the health care system. Finally, while acknowledging that health care professionals have a role to play as advocates for equality, non-discrimination, and justice, I argue that it is persons with mental disabilities themselves who have the right to exercise agency in their own lives and who, consequently, should be at the center of advocacy movements and the setting of the advocacy agenda.
Introduction
On October 3, 2008, The Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act was signed into law in the United States. This legislation introduced parity for mental health coverage for the first time in large group health insurance plans.1 Theoretically, this brought an end to a system in which it was legal for insurers to limit care for mental health and substance abuse conditions and to require patients to pay more out-of-pocket costs than are required for other medical conditions.2 The Act has been hailed as a progressive step toward removing inequities in access to and affordability of mental health care. At a political and public level, this may reassure those who live with serious mental disabilities and those who campaign for equality. The reality, however, is that the significant array of parity provisions at both the state and national levels constitute a major barrier for service users and clinicians in realizing real equality as an outcome of this legislation. The Act allows health insurers to determine which mental health and substance use conditions they will cover, to define for what conditions coverage is “medically necessary,” and to gain exemption from the law if providing mental health and substance use coverage increases their costs by 2% or more in the first year or by 1% or more in subsequent years. Furthermore, as Richard G. Frank, a health economist at Harvard Medical School, has observed, people with serious mental disabilities such as schizophrenia require many services, including psychosocial and occupational rehabilitation services, which are crucial to their recovery but are not provided for by the Act.3
Thus, legislation may be enacted to reduce or eradicate inequalities in health care, but statutes on their own often introduce only “formal equality” — that is, the law treats all individuals or health conditions alike. This is a superficial and deceptive form of equality, however, as there are many social, economic, and political factors at play that obstruct the translation of a law into the real, individual experience of equality. Formal equality alone gives an illusion that all are equal and that fairness exists, without addressing underlying inequalities in power, access, and socioeconomic and political circumstances.4 In this way, formal equality alone tends to perpetuate discrimination and inequality because it often fails to address real inequality in circumstances. Under a seemingly progressive veneer of respectability, disparities grow unchecked as public advocacy groups relax their activist efforts. Thus, far from bringing about progressive change, the introduction of equality legislation can have reactionary effects, exacerbating existing disparities in health access and care.
Within the human rights framework, it is imperative that we strive to achieve “substantive equality,” defined here as equality of opportunity, within the context of structural inequalities present in society. This means that circumstances that prevent the individual from achieving equality of opportunity must be addressed and that barriers to access and empowerment must be removed. Within health care, substantive equality does not guarantee equality of treatment outcomes, but it does guarantee equality of opportunity in trying to achieve those best outcomes.5
Mental disability and mental health care are surprisingly overlooked within the global discourse on health equality, and mental health has always appeared to be a side issue in both the public and academic health debate.6 There appears to be social distaste for issues pertaining to mental health and disability.
A significant exception to this attitude was the adoption of the United Nations Convention on the Rights of Persons with Disabilities on December 13, 2006.7 The Convention was negotiated during eight sessions of an Ad Hoc Committee of the General Assembly from 2002 to 2006. To date, there have been 140 signatories to the Convention (with 59 ratifications) and 83 signatories to the Optional Protocol (with 37 ratifications.) The Convention is intended as a human rights instrument with an explicit social development dimension:
It marks a paradigm shift in attitudes and approaches . . . from viewing persons with disabilities as ‘objects’ of charity, medical treatment and social protection towards viewing [them] as ‘subjects’ with rights, who are capable of claiming those rights and making decisions for their lives based on their free and informed consent as well as being active members of society.8
The Convention is broadly inclusive in terms of what is defined as disability, stating that “[p]ersons with disabilities include those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others.”9 Thus, the Convention constitutes a significant global commitment to a human rights framework in which issues of achieving substantive equality and the full and unfettered rights of persons with disabilities are placed at center-stage.
The importance of this Convention (as well as that of other recent regional declarations on mental disability) cannot be underestimated; mental disabilities are pervasive, common, and responsible for a significant proportion of disability, suffering, mortality, and lost productivity in human society. The social and economic “burden” borne by individuals, their families, their communities, and nations due to mental disability is enormous.10 Co-morbidity with physical illness and substance abuse is considerable.11 The relationship between mental disability and poverty, income inequality, social dislocation and alienation, and homelessness is well supported by growing evidence.12 Mental disability impacts education, social behavior, economic productivity, and cultural norms. Moreover, in the treatment of such conditions as HIV/AIDS and drug-resistant tuberculosis, mental disability is associated with high-risk behavior, poor treatment adherence, and inability to access care. In short, mental disability is a protean phenomenon whose often hidden tentacles extend into multiple areas of human experience and functioning. And yet, in both high-income countries (HICs) and low- and middle-income countries (LMICs) throughout the world, mental health care is a low priority, receiving stunted budgets, inadequate resources, and little attention from government.13 Globally, the integration of mental health into primary care is still in its infancy, while the skills, knowledge, and confidence of generalist health practitioners in managing mental disability are pitiful.14 In most countries, the level of mental health and substance use education and knowledge within the general public is minimal, if not negligible. Inequalities in mental health service development, provision, and access exist at all levels and in different contexts.15
The care, treatment, rehabilitation, and full integration of persons with mental disabilities is a complex challenge that cannot be met through the narrow confines of a purely biomedical or even public health model. The social, economic, cultural, and political factors that interact with innate and acquired biological processes in the genesis, course, and outcome of mental disabilities cannot be ignored in striving for equality. Efforts to improve global mental health will fail dismally if they are limited to the development of new drugs and therapeutic interventions. Likewise, attaining full human rights for persons with mental disabilities will never be achieved through a reliance on public health system reform alone.
Importantly, a human rights approach to mental disability requires a paradigm shift, as the Convention articulates, away from a public health approach in its conventional sense. A public health approach is inadequate, as it serves to reinforce paternalism and charity in identifying mental disability as a medical issue necessitating a medical “solution.” It views mental disability as a health issue only, requiring a health services response. In contrast, a rights-based approach to mental disability means acknowledging the social, economic, and political forces that result in the disability experienced by people with impairments. It also means ensuring that the principle of participation, as well as leadership by persons with disability in advocacy for substantive equality, is key to any international or domestic efforts to redress the inequalities and discrimination that exist in society. For health professionals involved in efforts to achieve real equality, a clinical role alone is ineffective. Instead, clinical expertise must be complemented by a commitment to an activist agenda in partnership with persons with mental disabilities — an agenda focused on bringing about change to the structural inequalities within social, economic, and political life that prejudice mental health, promote social exclusion, and retard recovery from mental disability.
Terminology and models of mental disability
The institutionalized medical language of mental disability is, at best, pejorative and situates mental conditions squarely within an individual disease framework. Terms such as “mental disease” and “mental disorder” construct psychological, emotional, and behavioral conditions as innate, biological, pathological states independent of socioeconomic, cultural, and political context. Likewise, the prevailing medical model of mental disability — which defines disability as an individual’s “restriction in the ability to perform tasks” and handicap as “the social disadvantage that could be associated with either impairment and/or disability” — serves to establish a direct causal relationship between individual impairment and disability.16 In contrast, the social model of disability, theorized by disabled activist and scholar Michael Oliver, views disability as something imposed upon persons by an oppressive and discriminating social and institutional structure and that is over and above their impairment.17
While the social model has characterized the disability movement and has been adopted as a basis for a human rights approach to disability, it is not beyond critique. For example, the British medical sociologist, Michael Bury, adheres to what he calls a socio-medical model of disability in which he reaffirms the reality of impairment in contributing to disability.18 In addressing the “causality” of mental disability, I am inclined to agree with Bury. Research has largely discredited a strict social model view of the causality of serious mental disability associated with such conditions as schizophrenia and bipolar illness to instead support a significant role for genetic and other biological factors in conferring vulnerability to these conditions. Importantly, this integrated, or multifactorial, view of the genesis of mental disability does not support the traditional medical or individual model either. In other words, a critique of the social model does not imply a return to the strict medical model that it superseded. Instead, what is consistent with current evidence from both the biological and sociological fields of research is a model of mental disability that integrates biological and social (as well as cultural and political) factors in establishing cause for these conditions.
The concept of “impairment” is not straightforward here. In terms of mental disabilities, impairment cannot be understood as a fixed structural or mechanical “abnormality” or “departure from human normality,” as Lorella Terzi expresses it.19 Innate or acquired genetic or biological factors associated with the origins of serious mental disabilities are not fixed impairments in the sense that blindness and spinal paralysis are. Rather, these factors exist as “vulnerability factors” — rendering the individual susceptible to psychosocial and environmental factors within society. Structural environmental forces act in concert with innate or acquired vulnerability factors over time to give rise to illness and disability. Complex reciprocal gene-environment interactions throughout neurodevelopment, involving both environmental mediation of gene expression and genetic influence over individual responses to environmental stressors, lie at the heart of most mental disabilities.20
Multiple levels of inequality and discrimination
A rights-based approach to mental disability needs to be informed by a clear analysis of the multiple levels of inequality and discrimination that exist in relation to individuals with mental disabilities both within and outside the health system. In a sense then, a “situation analysis” is required to illustrate the clear links that exist among social, economic, political, and cultural aspects of the environment and the origin, personal experience, and outcome of mental disabilities. The following discussion details how substantive inequality and discrimination characterize the manifestation and experience of mental disability in society as well as the provision of mental health care. While this analysis is intended to have global relevance, it contains an over-representation of data from the United States. This is not because that nation is alone in experiencing the inequalities cited, but rather, it is a reflection of the fact that significant research has been conducted in this field within the US, while there is a relative paucity of evidence available from other countries.
Unequal prevalence due to structural inequalities
In recent years it has become apparent that the prevalence of a number of mental disabilities varies in relation to social and economic disparities within societies. For example, systematic reviews show differences in both the prevalence and incidence of schizophrenia in relation to variables including urban versus rural status, social class, migration, unemployment, homelessness, and income inequality.21 In the case of schizophrenia, social and economic factors mediate expression of the condition in biologically vulnerable individuals.22 Such is the extent to which these factors impact negatively upon both the onset and outcome of schizophrenia that Brendan Kelly has invoked Paul Farmer’s concept of “structural violence” in relation to this illness.23 Kelly argues that social, economic, and political factors such as poverty and income inequality “shape both the landscape of risk for developing [schizophrenia] and the context in which health-care is provided.”24 He maintains that these forces constitute a form of “structural violence” that impacts the development and course of schizophrenic illness. Common mental disabilities such as anxiety, depression, and substance abuse also show an increased prevalence in relation to social class, unemployment, low income, homelessness, poverty, and income inequality.25 This means that individuals, families, and communities that occupy lower social classes, that are experiencing high levels of unemployment, and that are living in poverty also bear the burden of increased risk for mental disability along with all of its associated consequences. With respect to income inequality, it appears that health depends not just on personal income but also on the incomes of others in the society.26 While individual rank within the income distribution is undoubtedly important, it is clear that a large rich–poor gap within a community is bad for everyone in that community regardless of rank, not just for those at the bottom.
Unequal service access due to structural inequalities
Social and economic factors may serve as barriers to accessing mental health services in high-income countries as well as low- and middle-income countries. A community survey in the US (a high-income country), for example, reported that low-income individuals cited financial barriers to accessing care. However, this was not the case in the Netherlands or in Canada, both HICs, where economic disparities and income inequality are lower.27 Also in the US, a household survey of adolescents found that those of low-income status reported far more structural barriers to accessing mental health services than did their middle- and high-income counterparts.28 In LMICs, the impact of socioeconomic factors is likely to be greater.
The “treatment gap” (that is, the absolute difference between prevalence and percentage treated) for mental disabilities is significant worldwide and is due to a number of factors, including lack of knowledge about mental disabilities, stigma, lack of service availability, and socioeconomic barriers to accessing available services.29 An earlier study in Belize, for example, reported that 63% of individuals with schizophrenia, 89% of individuals with affective conditions, and 99% of individuals with anxiety conditions were untreated.30 The World Health Organization Mental Health Survey conducted in 14 countries found that 76–85% of individuals with serious mental disabilities in LMICs received no treatment, while 35–50% of those in HICs received treatment.31 Clearly, lack of treatment cannot be attributed solely to socioeconomic barriers to access — other likely reasons have already been mentioned. However, within LMICs like South Africa, it is patently obvious that poverty, disempowerment, and inadequate health education impede access to care. In such countries with high poverty and unemployment rates, those in need often cannot afford medical fees, the medicines prescribed, or the transport to convey them to clinics and hospitals. In such contexts, it is glaringly apparent how social and economic inequities lead to inequalities in access to care.
Unequal service access due to race, ethnicity, and gender
Racial and ethnic minorities in the United States are discriminated against in terms of their access to mental health services and appropriate treatments.32 Margarita Alegría and colleagues reported that of those who had depressive disorder in the previous year, more African Americans (59%), Latinos (64%), and Asians (69%) received no mental health treatment for depression compared with non-Latino whites (40%), while Daniel Rosen and colleagues found that nearly a quarter of white women (23%) with a mental disability received treatment as opposed to only 9% of African American women.33 In a sample of patients with schizophrenia living in the community, Richard Van Dorn and colleagues reported that significantly fewer African American patients had received atypical antipsychotics (the preferred therapy) than their white counterparts.34 Disparities in access to mental health services also exist with regard to gender. Women of low socioeconomic status have been shown to be at particular disadvantage in accessing mental health care, and there are clear barriers to accessing alcohol and substance abuse services for women compared with men.35 Furthermore, women diagnosed with borderline personality disorder encounter significant stigma and denial of access to optimal mental health care in comparison with women with other psychiatric diagnoses.36 There is a significant body of literature exploring the prejudices and discrimination that underlie the apparent gender bias in the diagnosis of this stigmatized “disorder.”
Unequal service access due to a diagnosis of mental disability
In many contexts in both HICs and LMICs, the diagnosis of mental disability itself creates a barrier for individuals in terms of future access to health care. Both real and perceived prejudice against the mentally disabled within the health sector is a potent barrier to accessing care. Graham Thornicroft argues that factors increasing the likelihood of treatment avoidance or delay before presenting for care include lack of knowledge about the features and treatability of mental disabilities, ignorance about how to access services, prejudice against people who have mental disability, and expectations of discrimination against people who have a diagnosis of mental disability.37 There is good evidence that real prejudices do exist within the health sector toward providing care for those with mental disabilities.38 Within some countries, the mentally disabled are still treated in abusive health care environments.39 There is also evidence that the mentally disabled receive unequal treatment for co-morbid physical disorders in comparison to their mentally well counterparts —meaning that a diagnosis of mental disability increases an individual’s risk of a poor outcome for co-morbid physical illness.40 Real and perceived discrimination contribute significantly to non-treatment, delays in accessing treatment, treatment non-adherence, and, ultimately, poorer outcomes.
Unequal funding and resource provision for mental versus physical disabilities
Globally, government funding for mental health services is disproportionately low compared with the burden of mental disability. Despite the fact that mental and substance use disabilities account for 12% of the global “burden” of disease, more than two-thirds of the world’s population lives in countries that spend less than 1% of their total public sector health budget on mental health services.41 Similarly, in many regions of the world, human resources for mental health care are severely limited in comparison with human resources for physical health care. Many countries, in both high-income and low- and middle-income contexts, report serious shortages of psychiatrists, psychologists, psychiatric nurses, and other mental health care professionals. This inequality in funding and service provision, in the face of the major burden of mental disability, represents global discrimination against mental disability and its care at the level of policy makers, health planners, and governments. Discriminating against those with mental disabilities by failing to pay for and provide care is particularly shortsighted as there are many effective and cheap interventions available that can be highly cost-effective in preventing co-morbidity, reducing disability, and returning mentally ill individuals to productive employment and social reintegration.
Unequal funding, resource provision, and protection from abuse across nations
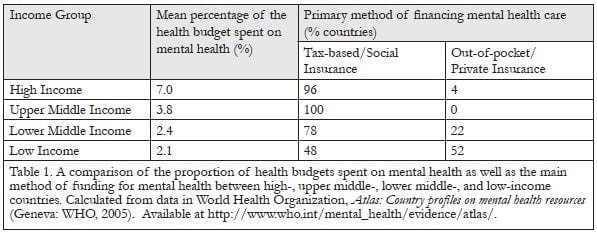
Low- and middle-income countries, which arguably support the bulk of the burden of mental disability, tend to spend less on mental health services than HICs. For example, of the 19 African countries for which data are available, 15 spend less than 1% of their health budgets on mental health.42 An additional inequality is the fact that it is very often the poorest people in the poorest countries who are required to make out-of-pocket payments for mental health care as their governments have made little or no provision for public funding of mental health services.43 Table 1 presents a comparison of the proportion of health budgets spent as well as the main method of funding for mental health among high-, upper middle-, lower middle-, and low-income countries. With respect to human resources, LMICs experience far greater shortages of mental health professionals than HICs. The average number of psychiatrists in HICs, for example, is 10.5 per 100,000 population, as opposed to low-income countries (LICs), where the average number is 0.05 per 100,000.44 The vast majority of HICs have established community mental health services, but only half of LMICs have this critical resource for mental health care.45 Furthermore, 20% of countries (all in the “developing world”) do not have basic antidepressant and antipsychotic medications available within their public health services, while the majority of LICs do not provide basic psychological therapeutic services for their citizens. Finally, whereas almost all high- and upper middle-income countries have legislated against abuse of the mentally disabled (both within and outside health care facilities), there are a significant number of lower middle- and low-income countries in which no such legislation has been passed. While it is conceded that legislation does not necessarily equate to an absence of abuse of the mentally disabled, it is nevertheless likely that a complete absence of legal protection is associated with more frequent occurrences of abuse. Certainly this has been the case in a number of LMICs without adequate mental health care legislation.46
A human rights approach to inequality and discrimination in relation to mental disability
The UN Convention sets out a framework for a rights-based approach to disability and in doing so “calls for changes that go beyond quality of care to include both legal and services reforms” and “demands that we develop policies and take actions to end discrimination in the overall society that has a direct effect on the health and well-being of the [mentally] disabled.”47 The Convention sets out a number of guiding principles:
- Respect for inherent dignity, individual autonomy including the freedom to make one’s own choices, and independence of persons;
- Non-discrimination;
- Full and effective participation and inclusion in society;
- Respect for differences and acceptance of persons with disabilities as part of human diversity and humanity;
- Equality of opportunity;
- Accessibility;
- Equality between men and women;
- Respect for the evolving capacities of children with disabilities and respect for the right of children with disabilities to preserve their identities.48
In addition to these principles, the Convention highlights the importance of a number of related rights. These include the following:
- Equal recognition before the law, access to justice, and legislative reform to abolish discrimination in society;
- Awareness-raising to educate society, combat prejudices and promote awareness of the capabilities of persons with disabilities;
- The right to life, liberty, and security of person including freedom from degrading treatment, abuse, exploitation, and violence;
- The right to movement, mobility, independent living, and full inclusion within the community including full access to and participation in cultural life, recreation, leisure, and sport;
- Freedom of expression and opinion, access to information, and full participation in political and public life;
- Respect for privacy, for the home and the family, including the freedom to make decisions related to marriage and parenthood;
- The right to equal education, work, and employment including the full accommodation of individual requirements;
- The right to health, habilitation, and rehabilitation;
- The right to an adequate standard of living, suitable accommodation, and social protection.49
With respect to mental disability, how does this framework inform our response to the inequities and discrimination present at multiple levels of society and mental health care? Specifically, if we take these principles and rights and apply them to the global “situation analysis” presented in the previous section, what actions are required to transform our societies so that persons with mental disabilities experience full equality, an end to discrimination, and full recognition of their personhood? I would propose that such an action plan at national as well as local levels include the following components:
- The development of a strong advocacy movement, led by persons with mental disabilities. Repeatedly it has been shown that “user-led” advocacy around issues of legal reform, services development, and societal transformation has been most effective in ending discrimination and stigmatization and achieving human rights for specific minority communities.50
- Legislative reform to abolish discrimination, to outlaw abuse and exploitation, and to protect personal freedom, dignity, and autonomy. Civil commitment laws that deprive individuals of their freedom “must provide for minimum substantive and procedural protections that protect mentally ill individuals’ fundamental agency.”51 In addition, such laws should guarantee the rights to counsel, appeal, and review in relation to involuntary commitment as well as redress for violations. As mentally disabled persons may not be in a position to safeguard their personal rights while unwell, there should be a mechanism for active monitoring and enforcement of such rights. In South Africa, for example, the Mental Health Care Act (2002) legislated for the establishment of independent regional “review boards” that are tasked with Ombuds office functions.52
- Legislative reform to enforce equality of opportunity, access, and participation in all aspects of life. While health-related legislative reform is important, this must be accompanied by legal measures aimed at rectifying inequalities and discrimination that exist with respect to the mentally disabled in social, economic, and political facets of society. Substantive equality requires attention to the social context that contributes to the origin of mental disabilities as well as to the use of mental health services by individuals.
- Inclusion of mental disability on the agenda of development programs and targets such as the Millennium Development Goals. At international, national, and regional levels, mental disability rights and “needs” must be included in programs aimed at achieving development targets and alleviating poverty and inequality — especially within LMICs.
- Mental health and social services reform with equitable funding for resources, infrastructure, and program development. Governments should be pressured to heed growing calls for the scaling up of health and social services relevant to mental disability as well as increased budget allocations for mental health.53 Signatories to the UN Convention and its Optional Protocol must be held accountable in terms of their domestic planning. The establishment of the Committee on the Rights of Persons with Disabilities as a monitoring organ means that citizens of States party to the Convention have a means of reporting local violations of the Convention and obtaining redress.54
- Removal of barriers to health services access encountered by persons with mental disabilities. Legal reforms such as The Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act are required within most nations to remove financial barriers to accessing services for those with mental disabilities.55 Legislation is also required to enforce equality and outlaw discrimination based on ethnicity, race, gender, and age within health services. Finally, education campaigns and programs on mental disability and the rights of mentally disabled persons should be conducted on an ongoing basis within all health services.
- Removal of barriers to accessing social, family-related, accommodation, educational, occupational, and recreational opportunities and to full participation for persons with mental disabilities. Legislative reforms, as well as public and institutional education campaigns and programs, should be implemented at national and local levels to remove these barriers to access, to eradicate stigma, and to ensure the full participation of persons with mental disabilities. Suitable accommodation is a fundamental right as enshrined in the Convention, and domestic policies, planning, and legal reform need to be informed by an acknowledgement of this right.
- Service systems reform to move away from institutional care toward providing treatment, care, rehabilitation, and reintegration within the community. As Alicia Eli Yamin and Eric Rosenthal state, “From a human rights perspective, people are entitled to live in and receive care in the community not because it is more efficient, but because all human beings develop their identities within social contexts, and have rights to work and study, as well as be with family and friends.”56 Furthermore, planning and decision-making power related to care in the community needs to be transferred to “the individuals and communities that the health system is supposed to serve.”57 This means the integration of “users” and family members into both national and local decision-making structures.
Conclusion
Mental disability and mental health care have been neglected in the global debate on health, human rights, and equality. Within the mental health field itself, much of the debate has been at a theoretical level, with a focus on stigma concepts and attitudes rather than on acts of discrimination and on strategies to change behavior.58 Graham Thornicroft and Aliya Kassam argue that stigma research in this field is, to some extent, “beside the point” as it tends to have focused on “hypothetical rather than real situations, shorn of emotions and feelings, divorced from context, indirectly rather than directly experienced, and without clear implications for how to intervene to reduce social rejection.”59 They call for a shift of focus from stigma to discrimination as this would place the mentally disabled in a position of parity with respect to anti-discrimination legislation and the human rights agenda.
The development of mental health policy and legislation within countries that have not established formal equality for mental disability is indeed a priority, and there are a number of global institutions actively engaged in this task.60 While highly necessary and laudable, these efforts to achieve formal equality should not stand alone, without similar advocacy focused on the achievement of substantive equality for persons with mental disabilities. Real life factors such as poverty; illiteracy; income inequality; homelessness; war and displacement; discrimination based on ethnicity, race, and gender; social exclusion; stigma; and abuse all impact the mentally ill individual’s ability to access services and realize full personhood within their communities. These factors also play a role in enhancing individual risk for mental disabilities and so, too, they act to hinder recovery and reintegration into social and occupational life.
A rights-based approach to mental disability means domesticating treaties such as the United Nations Convention on the Rights of Persons with Disabilities. Using the framework of this convention and others like it, it is possible to formulate an active plan of response to the multiple inequalities and discrimination that exist in relation to mental disability within our communities. While health care professionals arguably have a role to play as advocates for equality, non-discrimination, and justice, it is persons with mental disabilities themselves who have the right to exercise agency in their own lives and who, consequently, should be at the center of advocacy movements and the setting of the advocacy agenda. In support of this agenda, health care professionals need to become activists for the social and economic transformation of society into an environment in which those with mental disabilities can experience substantive equality.61
Jonathan Kenneth Burns, MBChB, MSc, FCPsych, is Senior Lecturer and Chief Specialist Psychiatrist in the Department of Psychiatry at the Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa.
Please address correspondence to the author c/o Department of Psychiatry, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, 4000, South Africa, email: burns@ukzn.ac.za.
References
1. For an excellent summary of the Act and its implications, see Harvard Medical School, “Benefiting from mental health parity,” Harvard Mental Health Letter (January 2009). Available at http://www.health.harvard.edu. For an overview of the historical background of this legislation, see C. L. Barry, “The political evolution of mental health parity,” Harvard Review of Psychiatry 14 (2006), pp. 185–194.
2. With respect to mental health, substance abuse conditions include a spectrum ranging from problematic abuse of alcohol and drugs to addiction to so-called “dual diagnosis” conditions (co-incidental substance abuse and mental disability where each compounds the negative impact of the other.)
3. Harvard Medical School (see note 1).
4. See S. Day and G. Brodsky, “Women’s equality: The normative commitment,” in S. Day and G. Brodsky (eds), Women and the equality deficit: The impact of restructuring Canada’s social programs (Ottawa: Status of Women Canada, 1998). Available at http://dsp-psd.pwgsc.gc.ca/Collection/SW21-32-1998E-1.pdf.
5. See Factum of the intervenor, Canadian Council of Disabilities. Part III (Point 6.) Available at http://www.ccdonline.ca/en/humanrights/promoting/andrews. For example, mental health is notably absent from the Millennium Development Goals (MDGs). For a critique, see J. J. Miranda and V. Patel, “Achieving the millennium development goals: Does mental health play a role?” PLoS Medicine 2/10 (2005), pp. 962–965. Miranda and Patel have pointed out that even though mental disability impacts, both directly and indirectly, many areas of social and economic life, mental health is completely absent from the MDGs. They provide evidence linking mental health directly to three of the MDGs — the eradication of extreme poverty and hunger, the reduction of child mortality, and the improvement of maternal health. However, if one considers the numerous effects of mental disability on social and economic development at the individual and community levels, then it is apparent that combating mental disabilities and reducing the morbidity associated with mental disabilities must contribute to the realization of almost all of the MDGs. The omission of mental health from the MDG agenda is a good example of the inequality and discrimination that exists within the health and development discourse itself.
7. The UN Enable website was established to report all aspects of the treaty and contains information on the guiding principles, entry into force, signatories, and monitoring of the Convention, as well as full-text versions of the Convention and its Optional Protocol in a number of languages. Available at http://www.un.org/disabilities/default.asp?navid=12&pid=150.
8. Ibid.
9. From the United Nations Convention on the Rights of Persons with Disabilities, Article 1, (2006), p. 4. Available at http://www.un.org/disabilities/default.asp?navid=12&pid=150 (see note 7).
10. Note: the use of the term “burden” here requires clarification. The term is not used in the sense of individuals being “burdensome” or a cause of hardship for others. The term is used to describe the added social and economic responsibilities and costs associated with either living with a mental disability or being in a care-giving role in relation to a person with a mental disability.
11. For a review of co-morbid mental disability and physical illness, see M. Prince, V. Patel, S. Saxena, et al., “No health without mental health,” Lancet 370 (2007), pp. 859–877. For discussion of co-morbid mental disability and substance abuse, with particular emphasis on developing LMICs, see R. Srinivasa Murthy, “Psychiatric comorbidity presents special challenges in developing countries,” World Psychiatry 3/1 (2004), pp. 28–30.
12. For a discussion of socioeconomic factors such as poverty and inequality and their effects on mental health, especially in LMICs, see V. Patel and A. Kleinman, “Poverty and common mental disorders in developing countries,” Bulletin of the World Health Organization 81/8 (2003), pp. 609–615.
13. The 2001 World Health Report was dedicated to mental health, documenting many of the inequalities that exist. For more information, see World Health Organization, World health report 2001. Mental health: New understanding, new hope (Geneva: WHO, 2001).
14. The World Health Organization and the World Organization of Family Doctors co-sponsored an investigation into the progress made in integrating mental health into primary health care. For the full report, see World Health Organization and World Organization of Family Doctors, Integrating mental health into primary care: A global perspective (Geneva: WHO, 2008).
15. The September 2007 volume of The Lancet contained a series of six papers documenting the current evidence related to global mental health, with a focus on LMICs. The second paper focused on resource scarcities and inequities. See S. Saxena, G. Thornicroft, M. Knapp, and H. Whiteford, “Resources for mental health: Scarcity, inequity, and inefficiency,” Lancet 370 (2007), pp. 878–889.
16. See M. Bury, “Defining and researching disability: Challenges and responses,” in C. Barnes and G. Mercer (eds), Exploring the divide: Illness and disability (Leeds: The Disability Press, 1996), pp. 17–38. Also see World Health Organization, The international classification of impairments, activities and participation (ICDH-2) (Geneva: WHO, 1980) for the prevailing medical model of disability.
17. See M. Oliver, Understanding disability: From theory to practice (Basingstoke: Palgrave, 1996), p. 32. According to Oliver, the social model “does not deny the problem of disability but locates it squarely within society.” Disability is “the disadvantage or restriction of activity caused by a contemporary social organization which takes no or little account of people who have … impairments and thus excludes them from participation in the mainstream of social activities.”
18. See M. Bury, “On chronic illness and disability,” in C. E. Bird, P. Conrad, and A. M. Fremont (eds), Handbook of medical sociology (5th edition) (New Jersey, PA: Prentice Hall, 2000), p. 179. Bury understands disability to be both biologically and socially caused — this giving rise to a conceptualization of disability that focuses on the interactions between individuals and their social location. For a discussion of sociological approaches to disability, see also C. Thomas, “How is disability understood? An examination of sociological approaches,” Disability and Society 19/6 (2004), pp. 569–583. For critiques of the social model of disability, see L. Terzi, “The social model of disability: A philosophical critique,” Journal of Applied Philosophy 21/2 (2004), pp. 141–157. See also C. Thomas, “Disability theory: Key ideas, issues and thinkers,” in C. Barnes, M. Oliver, and L. Barton (eds), Disability studies today (Cambridge, UK: Polity Press, 2002), p. 48. Lorella Terzi, whose work in educational philosophy focuses on disability and capability issues, quotes disability author Carol Thomas’s challenge of the materialist framework that underpins the social model of disability, arguing that the “materialist prioritization of the economic roots of disability” excludes other important dimensions of disability, such as the role of culture and cultural processes in shaping disabled persons’ position in society. Terzi also questions the validity of the “break-up of the causal link between impairment and disability, and the consequent causality established between society and disability.”
19. Terzi (see note 18).
20. For good reviews of the literature on gene-environment interactions during neurodevelopment and in relation to the causation of mental disabilities, see J. Van Os and P. Sham, “Gene-environment correlation and interaction in schizophrenia,” in R. M. Murray, P. B. Jones, E. Susser, et al. (eds), The Epidemiology of Schizophrenia (Cambridge, UK: Cambridge University Press, 2003.) Also see A. Caspi and T. E. Moffitt, “Gene-environment interactions in psychiatry: Joining forces with neuroscience,” Nature Reviews Neuroscience 7/7 (2006), pp. 583–590, as well as R. K. Lenroot and J. N. Giedd, “The changing impact of genes and environment on brain development during childhood and adolescence: Initial findings from a neuroimaging study of pediatric twins,” Developmental Psychopathology 20/4 (2008), pp. 1161–1175.
21. For systematic reviews of the prevalence and incidence of schizophrenia, see E. M. Goldner, L. Hsu, P. Waraich, et al., “Prevalence and incidence studies of schizophrenic disorders: A systematic review of the literature,” Canadian Journal of Psychiatry 47 (2002), pp. 833–843; and S. Saha, D. Chant, J. Welham, et al., “A systematic review of the prevalence of schizophrenia,” PLoS Medicine 2 (2005), p. e141. For a discussion on the relationship between schizophrenia and urbanicity, see L. Krabbendam and J. van Os, “Schizophrenia and urbanicity: A major environmental influence — conditional on genetic risk,” Schizophrenia Research 31 (2005), pp. 795–799. For evidence relating to schizophrenia and social class, see B. Cooper, “Schizophrenia, social class and immigrant status: The epidemiological evidence,” Epidemiologia e Psichiatria Sociale 14 (2005), pp. 137–144; and G. Harrison, D. Gunnell, C. Glazebrook, et al., “Association between schizophrenia and social inequality at birth: A case-control study,” British Journal of Psychiatry 179 (2001), pp. 346–350. For a meta-analysis and review of migration as a risk factor for schizophrenia, see E. Cantor-Graae and J. P. Selten, “Schizophrenia and migration: A meta-analysis and review,” American Journal of Psychiatry 162 (2005), pp. 12–24; for a comprehensive review of the literature on schizophrenia and employment, see S. Marwaha and S. Johnson, “Schizophrenia and employment,” Social Psychiatry and Psychiatric Epidemiology 39 (2004), pp. 337–349. For evidence on homelessness, see S. L. George, N. J. Shanks and L. Westlake, “Census of single homeless people in Sheffield,” British Medical Journal 302 (1991), pp. 1387–1389; and for a study linking income inequality to incidence of psychosis, see J. K. Burns and T. Esterhuizen, “Poverty, inequality and the treated incidence of first-episode psychosis: An ecological study from South Africa,” Social Psychiatry and Psychiatric Epidemiology 43 (2008), pp. 331–335.
22. For example, see S. Wicks, A. Hjern, D. Gunnell, et al., “Social adversity in childhood and the risk of developing psychosis: A national cohort study,” American Journal of Psychiatry 162 (2005), pp. 1652–1657.
23. Paul Farmer introduced the term “structural violence” to public health literature in relation to infectious diseases (in particular) and their relationship to social, political, and economic forces; see P. Farmer, Pathologies of power: Health, human rights and the new war on the poor (Berkeley, CA: University of California Press, Berkeley, 2005), pp. 40–50. Brendan Kelly applied the concept of “structural violence” to schizophrenia; see B. D. Kelly, “Structural violence and schizophrenia,” Social Science and Medicine 61 (2005), pp. 721–730.
24. Kelly (see note 23).
25. For reviews and evidence on the prevalence of mental disabilities in relation to social class, unemployment, low income, homelessness, poverty, and income inequality, see A. B. Ludermir and G. Lewis, “Links between social class and common mental disorders in Northeast Brazil,” Social Psychiatry and Psychiatric Epidemiology 36/3 (2001), pp. 101–107; T. Fryers, D. Melzer, and R. Jenkins, “Social inequalities and the common mental disorders: A systematic review of the evidence,” Social Psychiatry and Psychiatric Epidemiology 38/5 (2003), pp. 229–237; S. Weich and G. Lewis, “Material standard of living, social class, and the prevalence of common mental disorders in Great Britain,” Journal of Epidemiology and Community Health 52/1 (1998), pp. 8–14; S. Fazel, V. Khosla, H. Doll, et al., “The prevalence of mental disorders among the homeless in western countries: Systematic review and meta-regression analysis,” PLoS Medicine 5/12 (2008), p. e225; S. Weich, G. Lewis, and S. P. Jenkins, “Income inequality and the prevalence of common mental disorders in Britain,” British Journal of Psychiatry 179 (2001), pp. 222–227; R. S. Kahn, P. H. Wise, B. P. Kennedy, et al., “State income inequality, household income, and maternal mental and physical health: Cross sectional national survey,” British Medical Journal 321 (2000), pp. 1311–1315; and Patel and Kleinman (see note 12).
26. See I. Kawachi, S. V. Subramanian, and N. Almeida-Filho, “A glossary for health inequalities,” Journal of Epidemiology and Community Health 56 (2002), pp. 647–652.
27. See J. Sareen, A. Jaqdeo, B. J. Cox, et al., “Perceived barriers to mental health service utilization in the United States, Ontario and the Netherlands,” Psychiatric Services 58/3 (2007), pp. 357–364.
28. See P. W. Newacheck, Y. Y. Hung, M. J. Park, et al., “Disparities in adolescent health and health care: Does socioeconomic status matter?” Health Services Research 38/5 (2003), pp. 1229–1233.
29. See, for example, R. Kohn, S. Saxena, I. Levav, et al., “The treatment gap in mental health care,” Bulletin of the World Health Organization 82/11 (2004), pp. 858–866.
30. See J. Bonander, R. Kohn, B. Arana, et al., “An anthropological and epidemiological overview of mental health in Belize,” Transcultural Psychiatry 37 (2000), pp. 57–72.
31. The World Health Organization Mental Health Survey was conducted by a consortium from many countries throughout the world, yielding much valuable data. See WHO World Mental Health Survey Consortium, “Prevalence, severity, and unmet need for treatment of mental disorders in World Health Organization World Mental Health Surveys,” Journal of the American Medical Association 291/21 (2004), pp. 2581–2590.
32. For evidence on racial and ethnic discrimination in mental health care, see M. Alegría, P. Chatterji, K. Wells, et al., “Disparity in depression treatment among racial and ethnic minority populations in the United States,” Psychiatric Services 59/11 (2008), pp. 1264–1272; and D. Rosen, R. M. Tolman, L. A. Warner, et al., “Racial differences in mental health service utilization among low-income women,” Social Work and Public Health 23/2–3 (2007), pp. 89–105.
33. Ibid.
34. See, for example, R. A. Van Dorn, J. W. Swanson, M. S. Swartz, et al., “The effects of race and criminal justice involvement on access to atypical antipsychotic medications among persons with schizophrenia,” Mental Health Services Research 7/2 (2005), pp. 123–134.
35. For an Irish study showing unequal access to mental health services for women of low socioeconomic status, see G. Luddy, “Women, disadvantage and health,” Irish Medical Journal 100/8 (2007), pp. 71–73. For evidence that women are disadvantaged in accessing alcohol treatment services, see C. Weisner and L. Schmidt, “Gender disparities in treatment for alcohol problems,” Journal of the American Medical Association 268/14 (1992), pp. 1872–1876.
36. For an excellent discussion of gender issues underlying the borderline personality disorder diagnosis, see N. Nehls, “Borderline personality disorder: gender stereotypes, stigma, and limited system of care,” Issues in Mental Health Nursing 19/2 (1998), pp. 97–112.
37. See G. Thornicroft, “Stigma and discrimination limit access to mental health care,” Epidemiologia e Psichiatria Sociale 17/1 (2008), pp. 1–9.
38. For a review of stigma experienced within the health services by people with mental disability, see D. Lawrence and R. Coghlan, “Health inequalities and the health needs of people with mental illness,” NSW Public Health Bulletin 13/7 (2002), pp. 155–158.
39. See, for example, D. L. Mkize, “Human rights abuses at a psychiatric hospital in KwaZulu-Natal,” South African Journal of Psychiatry 13/4 (2007), pp. 137–142; and Mental Disability Rights International and Center for Legal and Social Studies, Ruined lives: Segregation from society in Argentina’s psychiatric asylums (Washington, DC: Mental Disability Rights International, 2007). Available at http://www.mdri.org/PDFs/reports/MDRI.ARG.ENG.NEW.pdf.
40. For discussion of differential care of co-morbid physical illness in those with mental disabilities within HICs, see A. Bahm and C. Forchuk, “Interlocking oppressions: The effect of a comorbid physical disability on perceived stigma and discrimination among mental health consumers in Canada,” Health and Social Care in the Community 17/1 (2009), pp. 63–70; and M. M. Desai, R. A. Rosenheck, B. G. Druss, et al., “Mental disorders and quality of diabetes care in the veterans health administration,” American Journal of Psychiatry 159/9 (2002), pp. 1584–1590.
For similar discussion and evidence from LMICs, see A. Cohen, V. Patel, R. Thara, et al., “Questioning an axiom: Better prognosis for schizophrenia in the developing world?” Schizophrenia Bulletin 34/2 (2008), pp. 229–244.
41. See World Health Organization, Mental health fact sheet (2009). Available at http://www.who.int/mental_health/en/index.html; and A. A. Shah and R. H. Beinecke, “Global mental health needs, services, barriers and challenges,” International Journal of Mental Health 38/1 (2009), pp. 14–29. For an excellent interactive database on the WHO website containing a range of data on mental health systems in over 100 countries, see World Health Organization, Atlas: Country profiles on mental health resources (2005). Available at http://www.who.int/mental_health/evidence/atlas/.
42. Shah and Bienecke (see note 41).
43. World Health Organization (2005, see note 41).
44. Shah and Bienecke (see note 41).
45. For a review, see G. Thornicroft and M. Tansella, “Components of a modern mental health service: A pragmatic balance of community and hospital care. Overview of systematic evidence,” British Journal of Psychiatry 185/4 (2004), pp. 283–290.
46. Mkize (see note 39); and Mental Disability Rights International and Center for Legal and Social Studies (see note 39).
47. See A. E. Yamin and E. Rosenthal, “Out of the shadows: Using human rights approaches to secure dignity and well-being for people with mental disabilities,” PLoS Medicine 2/4 (2005), pp. 296–298.
48. United Nations Enable (see note 7).
49. Ibid.
50. See D. Goodley, “Empowerment, self-advocacy and resilience,” Journal of Intellectual Disability 9/4 (2005), pp. 333–343.
51. Yamin and Rosenthal (see note 48).
52. For an online version of the South African Mental Health Care Act (2002), see http://www.acts.co.za/mental_health_care_act_2002.htm.
53. See Lancet Global Mental Health Group, “Scale up services for mental disorders: A call for action,” Lancet 370/9594 (2007), pp. 1241–1252.
Normal
0
false
false
false
EN-US
X-NONE
X-NONE
/* Style Definitions */
table.MsoNormalTable
{mso-style-name:”Table Normal”;
mso-tstyle-rowband-size:0;
mso-tstyle-colband-size:0;
mso-style-noshow:yes;
mso-style-priority:99;
mso-style-parent:””;
mso-padding-alt:0in 5.4pt 0in 5.4pt;
mso-para-margin:0in;
mso-para-margin-bottom:.0001pt;
mso-pagination:widow-orphan;
font-size:10.0pt;
font-family:”Times New Roman”,”serif”;}
54. UN Enable (see note 7).
55. Harvard Medical School (see note 1).
56. Yamin and Rosenthal (see note 48).
57. Ibid.
58. See G. Thornicroft and A. Kassam, “Public attitudes, stigma and discrimination against people with mental illness,” in C. Morgan, K. McKenzie, and P. Fearon (eds), Society and Psychosis (Cambridge, UK: Cambridge University Press, 2008), pp. 179–197.
59. Ibid.
60. For a discussion of policy development within Africa, see O. Gureje and A. Alem, “Mental health policy development in Africa,” Bulletin of the World Health Organization 78/4 (2000), pp. 475–482. The WHO is actively engaged in projects to promote the development of mental health policy and legislation around the globe (with an emphasis on LMICs.) For an excellent WHO resource, see World Health Organization, WHO resource book on mental health, human rights and legislation (2005). Available at http://www.who.int/mental_health/policy/legislation/essentialpackage2v1/en/index.html. An important platform for promoting the scaling up of mental health services globally is the Movement for Global Mental Health. For a variety of resources, see the MGMH website at http://www.globalmentalhealth.org/articles.php?id=72.
61. For a discussion, see M. Donohoe, “Roles and responsibilities of health care professionals in combating environmental degradation and social injustice: Education and activism,” Monash Bioethics Review 27/1–2 (2008), pp. 65–82.