The right to sutures: Social epidemiology, human rights, and social justice
Sridhar Venkatapuram, Ruth Bell, and Michael Marmot
Health and Human Rights 12/2
Published December 2010
Abstract
The article examines the convergences and contrasts between social epidemiology, social medicine, and human rights approaches toward advancing global health and health equity. The first section describes the goals and work of the WHO Commission on Social Determinants of Health. The second section discusses the role of human rights in the Commission’s work. The third section evaluates, from the perspective of social epidemiology, two rights-based approaches to advancing health and health equity as compared to a view that focuses more broadly on social justice. The concluding section identifies four areas where social epidemiologists, practitioners of social medicine, and health and human rights advocates can and must work together in order to make progress on health and health equity.
Introduction
Each of three fields — health and human rights, social medicine, and social epidemiology — has valuable insights, and professionals working in these fields hold important roles in advancing the health of people in society. In particular, despite the comparatively recent establishment of the health and human rights field, it has made an enormous contribution to the advancement of global health equity. It has done so by providing an analytical framework to identify and protect the most vulnerable anywhere in the world from poorly conceived public health policies as well as from the egregious abuses that make them vulnerable to ill health and mortality. While health and human rights advocates have from the start taken a global perspective, social medicine and social epidemiology have been slower to catch up. Advancing global health and health equity against a wide variety of threats — including abusive actors, unjustifiable reasoning, and plain complacency of those who have the power to make a difference — will require coherent reasoning and coordination across the fields of social epidemiology, social medicine, and health and human rights. So it is welcome and commendable that this journal, the original publication of the health and human rights field, is taking the lead toward building such coherence and cooperation with a special issue on social determinants of health.
In this article, we examine the convergences and contrasts between social epidemiology, social medicine, and human rights approaches toward advancing global health and health equity. For the purposes of this article, we understand social medicine to be the practice of clinical medicine in a manner that demonstrates social awareness, while social epidemiology is the study of the social distribution of disease and causes of that distribution across groups and individuals. The first section of the article describes the goals and work of the WHO Commission on Social Determinants of Health. The second section discusses the role of human rights in the Commission’s work. The third section evaluates, from the perspective of social epidemiology, two rights-based approaches to advancing health and health equity in comparison to a view that focuses more broadly on social justice. The article concludes by identifying four areas where social epidemiologists, practitioners of social medicine, and health and human rights advocates can and must work together in order to make progress on health and health equity.
The Commission on Social Determinants of Health
The WHO Commission on Social Determinants of Health (“the Commission”) was set up in 2005 by the late J. W. Lee, then Director-General of the World Health Organization, with the mission to collect and synthesize global evidence on the social determinants of health, assess their impact on health inequity, and make recommendations for action to address that inequity.1 Members of the Commission and its secretariat were motivated by three driving forces: a belief in social justice, respect for evidence, and frustration that there was far too little action on the social determinants of ill health and health inequalities. These powerful motivating forces led to three years of detailed work compiling and analyzing research, consulting with experts from around the world as well as across many disciplines and professions, meeting with governments and practitioners, and producing a final report and recommendations.2 Rather than being an end in itself, the work of the Commission and the resultant report, Closing the gap in a generation: Health equity through action on the social determinants of health (hereafter Final Report) is meant to instigate discussions within institutions and the public sphere and help promote social action and policies to advance health and health equity, both within countries and transnationally.
Based on the collected evidence, the Commission made its recommendations across three overarching areas for action. The first is “to improve the conditions of daily life — the conditions in which people are born, grow, live, work and age.”3 The second is to tackle the “structural drivers of those conditions,” that is, the inequitable distribution of power, money, and resources. The third is to “measure the problem, evaluate action, expand the knowledge base, develop a workforce that is trained in the social determinants of health, and raise public awareness about the social determinants of health.” Within these areas of action the Commission made further recommendations in twelve areas: 1) early child development and education, 2) healthy places — the living environment, 3) fair employment and decent work, 4) social protection across the life course, 5) universal health care, 6) health equity in all policies, 7) fair financing, 8) market responsibility, 9) gender equity, 10) political empowerment, 11) good global governance, and 12) knowledge, monitoring, and skills. The Commission’s recommendations are necessarily broad given its global remit and the very different contexts in which people live their lives around the world. At the same time, the broad principles embodied in the recommendations are relevant to and applicable in all contexts. Developing national or regional strategies to improve health equity requires contextual analysis across the areas identified by the Commission. Indeed, the resolution agreed at the World Health Assembly in May 2009 urges all member states to tackle health inequities through action on the social determinants of health and to assess the impact of policies and programs on health inequities.4 A number of countries and regions around the world are in the process of taking up the Commission’s recommendations and translating them to suit their national and regional circumstances, including England, a number of European countries, Brazil, Argentina, Chile, Sri Lanka, Thailand, and the Canadian provinces of Manitoba and Quebec.
The Commission’s recommendations are rooted in an analytical causal framework that is based on the intersection of three sets of social dynamics as they relate to conditions of daily life. The first is that the conditions of daily life in which individuals are born, grow, live, work, and age determine their incidence of disease, their experience of morbidity, and length of lifespan. Second, these daily living conditions include proximal determinants such as exposure to harmful substances and biological organisms, the availability of material needs such as food, potable water, and shelter, and the social environments that affect psychobiological pathways and health-related behaviors. Third, these daily conditions also have distal structural drivers or “causes of causes” — the economic, social, and political conditions that together with background social and cultural norms create and distribute the proximate causes across individuals and social groups.
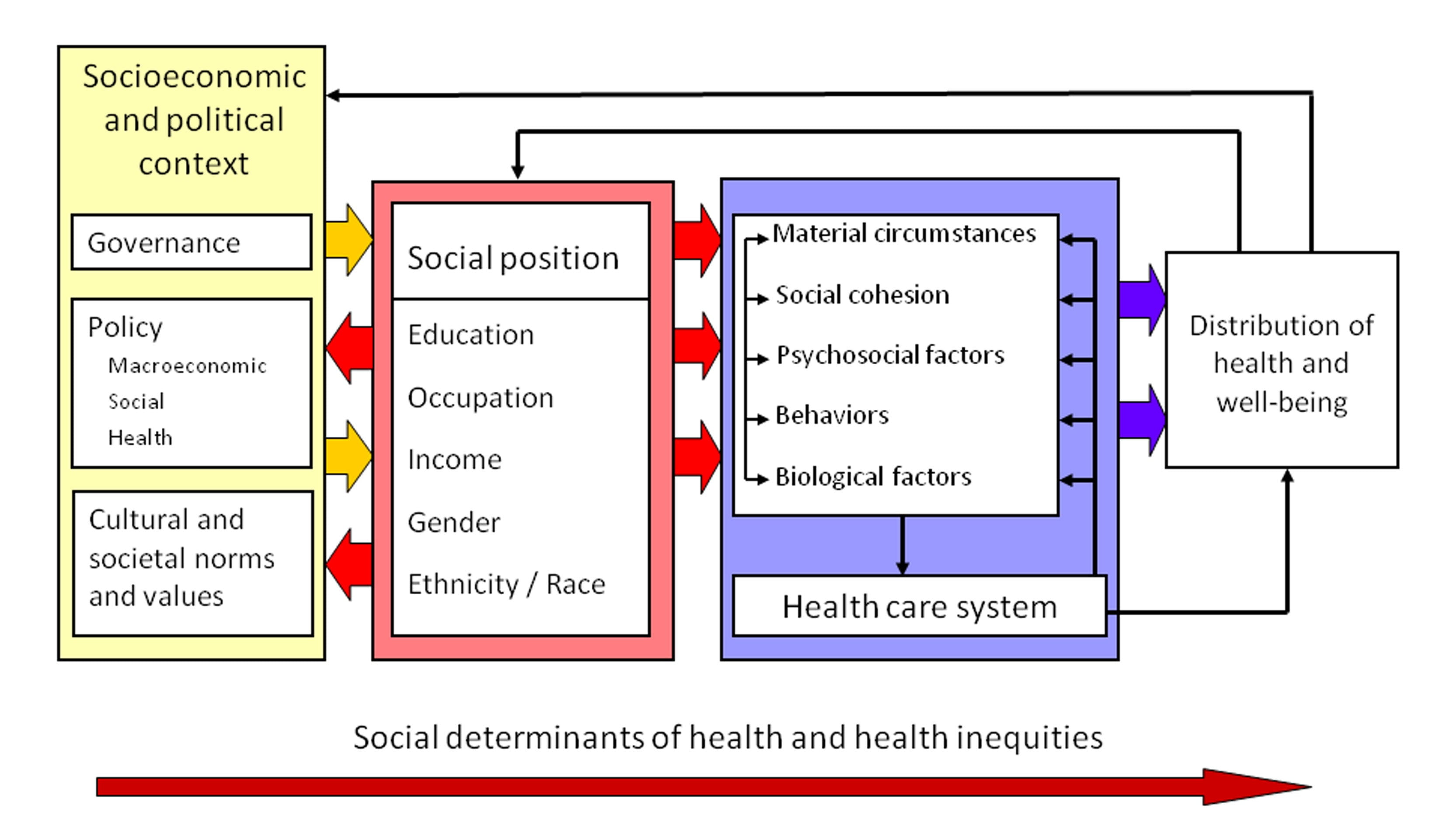
In other words, poor health and health inequalities across individuals and social groups are brought about by multiple and multi-level factors that interact in complex ways. These factors include the individual material circumstances in which people live their lives as well as social cohesion and psychosocial, behavioral, and biological factors, and the functioning of the health care system. The way people interact with or experience these factors is determined by their position in the social hierarchy along dimensions of wealth and income, occupation, education, gender, race or ethnicity, and geographical location of residence. All these causal factors are in turn affected by a political, economic, social, and cultural context that determines the unequal distribution of power, prestige, and resources. Figure 1 is a diagram of the Commission’s conceptual framework.
The Commission’s analysis reflected the intellectual and disciplinary traditions of social epidemiology and social medicine. Social epidemiology begins with observations and measurements of the distribution of health across social groups differentiated by factors such as occupation, income, education, gender, ethnicity/race, age, and geographical area. This then allows for the identification of the supra-individual determinants of health and their distribution, and for an understanding of the causal chain from social, economic, and political drivers to differential health outcomes in individuals and social groups. The Commission’s recommendations for action to improve individual health and the distribution of health are grounded in identifying the causal chain, based on empirical evidence. At the core of the Commission’s view is the understanding that individual health — and the distribution of health achievements across groups — is significantly influenced by determinants outside the health care system as well as by the functioning of the system itself. As a result, the Commission identified universal primary health care as one important area for social action, but it is just one of the Commission’s twelve recommended areas for action to improve health and health equity.
Figure 1. Commission on Social Determinants of Health conceptual framework
Source: Commission on Social Determinants of Health, Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report on Social Determinants of Health (Geneva: World Health Organization, 2008), p. 43. Available at http://whqlibdoc.who.int/publications/2008/9789241563703_eng.pdf. Amended from O. Solar and A. Irwin, “A conceptual framework for action on the social determinants of health,” in Disscussion paper for the Commission on Social Determinants of Health (Geneva: World Health Organization, 2007). Available at http://www.who.int/social_determinants/resources/csdh_framework_action_05_07.pdf. Reprinted with permission.
Social medicine begins from the recognition of the impact of social and economic conditions on access to, and experience of, medical care as well as their direct impact on health achievements. Therefore, social epidemiology and social medicine share the recognition of the social determinants or social bases of health and health inequalities. Indeed, the only thing that could be said to distinguish social epidemiology and social medicine is the extent to which medical care is given importance in the analysis of the social causation and distribution of health and longevity. Put in another way, social epidemiologists are practitioners or supporters of social medicine, and practitioners of social medicine are social epidemiologists, but the scope of social epidemiology is broader than medical care. The broader the scope of social medicine’s analysis of the social conditions affecting health and its distribution, the less social medicine can be distinguished from social epidemiology. Given this understanding of the relationship between social medicine and social epidemiology, it should be clear that the tradition of social medicine greatly informed the work of the Commission, not least by many of the individuals involved who consider themselves to be practitioners of social medicine.
The gap, the gradient, and social justice
The starting position of the Commission was that there is no inherent biological or “natural” explanation for the gross inequalities in health achievements we see between countries and within countries. There is no inherent biological reason why life expectancy for a girl born in Japan is 86 years, while for a girl born in Sierra Leone it is 43 years. Nor is there a biological explanation for why the maternal mortality ratio in Sierra Leone is 2,100 deaths per 100,000 live births while in Ireland the ratio is 1 maternal death per 100,000 live births.5 In the case of Malawi, Paul Farmer identifies the lack of sutures, sterile drapes, and anesthesia among the many reasons for the unacceptably high maternal mortality ratio.6 The Commission concerns itself with such lack of necessary medical supplies — as part of the conditions of daily living — and with the upstream causes of such conditions of daily living. Like Farmer, the Commission asks: how can these conditions be improved through social action?
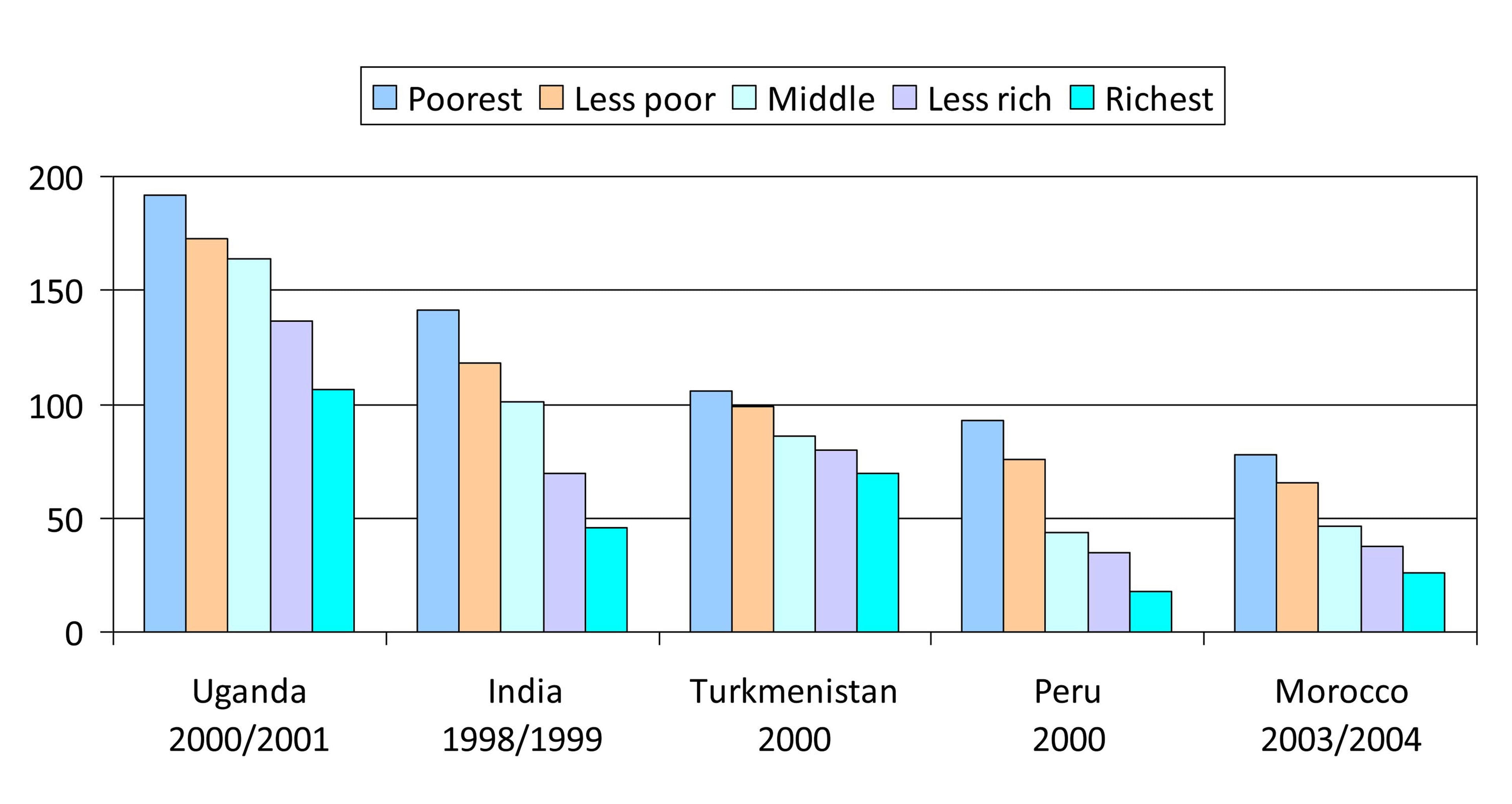
In its Final Report, the Commission presented evidence that the systematic differences in health achievements between countries and within countries across groups stratified by education, income, occupation, gender, ethnicity, race, and geographical area of residence are determined by social, political, and economic policies and practices. This evidence militates against analyses that focus narrowly on biological processes at the individual level in a contextual vacuum. One piece of compelling evidence can be found, for example, by examining under-five mortality against household wealth in developing countries (Figure 2). The difference in mortality levels within each country illustrates one detail of the scale of inequality in this indicator, with a substantial gap between the best and the worst off and, importantly, a step-wise gradient across the whole society.
The Commission argues that systematic differences in health achievements that are avoidable or preventable by reasonable means are unfair; they are health “inequities.” To return to Paul Farmer’s example, reducing maternal mortality through the provision of sutures certainly falls into the category of reasonable means in that it is both practically possible to provide sutures and providing sutures is neither morally offensive nor unreasonable. The same is true of many interventions that would make significant improvements in the conditions of daily living (the circumstances in which people are born, grow, live, work, and age). Indeed, a major source of the frustration driving the Commission’s work to collect evidence was the recognition of how much health and health equity could be improved through reasonable means in contrast to the poor reasoning and complacency of many societies and international institutions.
Based on collected evidence and its analysis of the causation and distribution of ill health, the Commission adopted the view that taking action to reduce health inequities is a matter of social justice. The Commission states, “Achieving health equity within a generation is achievable, it is the right thing to do, and now is the right time to do it.”7 This is not meant to be hollow rhetoric. Any meaningful understanding and commitment to the idea of social justice entails addressing manifest injustices, and such manifest injustices exist where reasonable means could be deployed to alleviate disproportionate ill health or prevent mortality. This social justice imperative applies to improving the health of those who suffer most egregiously as well as improving the health of those represented by the gradient, the remaining majority of the population. In light of the unprecedented intellectual and material resources that exist in the world today, the goal of social action, in principle, should be to flatten the social gradient in health by leveling up health outcomes across the social spectrum so that all are capable of achieving the health of the healthiest. This is what is meant by “closing the gap in a generation.”
Figure 2. Under-5 mortality rate per 1000 live births by level of household wealth.
Source: Commission on Social Determinants of Health, Closing the gap in a generation: health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health (Geneva: World Health Organization, 2008), p. 30, using DHS data adapted from D. R. Gwatkin, S. Rutstein, K. Johnson, et al., Socio-economic differences in health, nutrition, and population within developing countries: An overview, Country Reports on HNP and Poverty (Washington: World Bank, 2007). Reprinted with permission.
Is closing the gap in a generation feasible?
Numerous epidemiological studies have shown that gaps and gradients in health can vary significantly between countries and within countries over time, and there have been natural experiments that also provide valuable information. We know, therefore, that average measures of population health and the distribution of health are susceptible to social and political action. For example, with the deep political, social, and economic changes that followed the dissolution of the former USSR, average population health measures worsened, and the gradient in adult mortality by education steepened in Russia since the 1980s.8 In New Zealand, “indigenous inequalities,” that is, measurable health inequalities between mortality rates of the indigenous and non-indigenous populations, widened between the mid-1980s and the mid-1990s following a period when structural adjustment policies were introduced and social and income inequalities increased. These inequalities then narrowed following the introduction of pro-equity policies and health reforms in the late 1990s.9 Prevalence of certain chronic diseases is lower among low-income residents in the Canadian province of Quebec, which instigated an anti-poverty strategy in 2002, than in equivalent populations in other Canadian provinces that did not have such a policy.10 Studies comparing Nordic countries with other developed countries associate generous and universal social welfare policies with lower levels of poverty and better outcomes for disadvantaged people.11 While these findings do not demonstrate direct causality, there is a plausible causal chain linking political decisions and social action to changes in the health of entire populations and lower socioeconomic groups. We have evidence that the absolute levels and social gradient of health achievements can rapidly worsen within a single generation.12 The Commission asserts that health and health equity could also improve dramatically in a single generation if and when appropriate social action is taken within and across countries.
The Commission and human rights
From the start, the Commission based its work on an awareness of human rights and the relationship between human rights and health. It also built on opportunities to discuss with human rights experts — including Paul Hunt, the former United Nations Rapporteur on the Right to Health — the possible role of international human rights law in the Commission’s analysis and Final Report. While it was clear that human rights law would be an important part of implementing the Commission’s recommendations, members of the Commission were not convinced that explicit consideration of the legal human right to health changed their final causal analysis. That is, to what extent can the violation of human rights — as defined by international statutes — explain the (social) causation and distribution of ill health and mortality? On the one hand, all the social determinants identified thus far in the causal chain of ill health and mortality could conceivably be recast as violations of human rights. Such recasting without providing the underlying epidemiological information and analysis would not in and of itself supply convincing evidence of causation. Further, providing epidemiological evidence with accompanying human rights legal analysis does not provide additional explanatory value. After epidemiological analysis, however, human rights law has immense value in guiding how societies must act in order to protect, promote, and fulfill the rights implicated in the social epidemiological analysis. The Commission said as much in the Final Report by stating that the right to health as set out by Paul Hunt’s report presents a compelling case for action on the social determinants of health. On the other hand, it is not immediately clear how a human rights analysis of health can capture some of the central findings in social epidemiology, namely, the observations about the health of social groups and the broad social gradient in health within and across countries.
When evaluating the role of human rights in the Commission’s analysis and recommendations, one also must bear in mind that the Commission was very aware that within the WHO and in the global health policy arena, the two dominant approaches to analyzing poor health and health inequalities focus on medical interventions/health systems or economic policy. The focus on disease prevalence and medical care/health systems aims to address ill health through the provision of medical interventions such as vertical programs or better functioning of health systems broadly conceived. And the perspective of economics, exemplified by the WHO Commission on Macroeconomics and Health, focuses on improving the cost-effectiveness of health systems in order to improve economic growth while also being mindful of the health needs of the “ultra” income-poor. The Commission championed an alternative framework of analysis that presented evidence of the full breadth of social determinants of health beyond that generally considered within the realm of medical interventions/health systems. The Commission also argued that all avoidable ill health and health inequalities must be addressed as a matter of social justice, not just those factors instrumental to economic growth.
Furthermore, the Commissioners were well aware that the social distribution of ill health and health achievements is a secondary concern in both the focus on controlling diseases and mortality through medical interventions and in investing in health for economic growth. It is quite conceivable that average indicators of health or economic growth targets could be reached through focusing on improving the health achievements of the more advantaged in societies. This is why equity and social justice are concerns that run throughout the Commission’s analysis. Finally, but not least important, the Commission wanted to show that the health of individuals in both rich and poor countries could be evaluated within one framework of analysis, that the preventable deaths and suffering of the disadvantaged and the social gradient as it affects health in both rich and poor countries are the result of the way in which we organize our societies through economic, social, and political policies and practices.13 For these reasons and more, the Commission drew largely on the methods of social and natural sciences research in order to analyze the causes and distribution of ill health and mortality within and across countries.
Nevertheless, the idea of human rights and entitlements came to the fore throughout the Commission’s discussions. Dr. Ricardo Lagos, former President of Chile and a member of the Commission, pointed out that Chile has introduced a system of social guarantees, or entitlements to health care, for a number of health conditions as rights of citizenship. Mirai Chatterjee, a Commission member from India, described how the Self Employed Women’s Association campaigned and won legal rights for poor women in Ahmedabad to work as street market traders.14 So the ideas of human rights as well as rights and entitlements were present throughout the functioning of the Commission and appear in the Final Report. At the same time, the Commissioners and others would assert that human rights do not encompass the entirety of the idea of social justice. Advancing health and health equity as a matter of social justice will entail promoting, protecting, and fulfilling human rights, including the right to health, as well as taking additional social action. Moreover, in thinking about health and social justice, the Commission recognized an affinity between Amartya Sen’s ethical arguments for seeing social justice as the expansion of freedoms and social epidemiological research on the effects on health of having control, autonomy, and ability to participate in social relationships.15 Indeed, Sen’s thinking was influential in setting up the Commission and he served as one of the Commissioners. Expanding on Sen’s line of reasoning, the Commission positioned the concept of empowerment for individuals, communities, and nations across three dimensions — material needs, psychosocial factors (having control over one’s life), and political voice and participation in decision-making processes — as fundamental to making progress toward health equity.
In responding to the Commission’s Final Report, some human rights advocates such as Paul Hunt and Mary Robinson have remarked that it should have granted a larger and far more central role to human rights.16 Received in the positive and constructive manner that Hunt and Robinson intended, these comments have been understood to mean that there is much more unexplored potential in bringing together human rights analysis and social epidemiology/social medicine. For example, the role of legal institutions, particularly those institutions that protect constitutional and international human rights, may have distinct contributions to make in addressing certain social determinants of health or for establishing social norms. Indeed, no modern approach to health and human rights would exist without the legal institutions that have established human rights law. Although the Commission has formally concluded its activities, as part of the follow-on activities, there have been efforts to think more concertedly on integrating social epidemiology/social medicine and human rights. In the next section, we present some of the initial analysis of the convergences and contrasts between social epidemiology/social medicine approaches and human rights-based approaches. While we identify a divergence at the point of causal analysis of health, we argue these approaches are not only convergent — in the sense that they both have common concern and push toward the same goal of greater health equity — but that they are also interdependent and must work together in order to advance health and health equity within and across countries. As concrete illustration of our reasoning about how social epidemiology/social medicine and human rights approaches can and should be integrated and jointly deployed to advance health and health equity, we have taken the liberty of focusing on Paul Farmer’s rhetorical question in an earlier issue of this journal, “Should there be a right to sutures?”17
Human rights and social justice
In describing a visit to Malawi, Farmer reported the maternal mortality ratio in Malawi as being a shocking 1,800 per 100,000 live births. He described how the two obstetricians in a maternity hospital faced severe shortcomings in supplies, facilities, and personnel compared with the Harvard teaching hospitals where Farmer works part of the year. However, as a result of the efforts of the two Malawian obstetricians, the maternal mortality ratio within the hospital was reported to be 300 per 100,000 at the time of his visit. Given that this within-hospital maternal mortality ratio is still deplorably high, the fact that it could be seen as a consolation that it was one-sixth of the national ratio left Farmer speechless. Tarek Meguid, one of the obstetricians who showed Farmer around the hospital, described the lack of material resources — of supplies, facilities, and personnel — in terms of human rights abuses. Farmer, in turn, asked readers “Should there be a right to sutures? To sterile drapes? To anesthesia?”18
Most readers would likely answer with a resounding “Yes, of course!” And yet, Farmer’s questions raise one of the central conceptual problems in the health and human rights paradigm: how to frame a right to something that is not explicitly identified in human rights law? How to reconcile an understanding of the often dire health situation “on the ground” with the formal texts of human rights law is a dilemma for which even those deeply committed to the ideals of human rights often pursue remarkably different paths in order to advance global health and health equity. Even among human rights advocates, (putting aside the views of the skeptics and critics of human rights), if a particular right to something does not appear in the legal documents, then such a human right does not exist. But what if one believes, for example, that the provision of sutures is not only a reasonable and feasible means to prevent deaths but that it should be seen as a human right? In the following discussion, we frame this issue as one that may be addressed by pursuing three possible paths. Each path is a potential answer when faced with this not-so-uncommon situation, where the identification of the causal pathways to ill health and mortality on the ground is sought to be integrated with the idea and law of human rights.
Path 1 would offer the choice to continue to engage with international human rights law and with attempts to interpret the existing law via documentation, reporting, and various avenues of enforcement with the goal of addressing the missing cause or treatment, such as in the example of the provision of sutures. Path 2, rather than seeking formal engagement with human rights law, would seek to derive principles and values from human rights law and infuse them into health programs and interactions between individuals on the ground. Finally, Path 3 would in fact back away from the arena of human rights law and would instead attempt to bridge the analysis of the causes and distribution of ill health and mortality on the ground with ethical reasoning about social justice. Out of such ethical reasoning — informed by evidence of the causes, inequalities, and consequences of ill health — could arise arguments for advancing rights and other types of social action. The three paths are not mutually exclusive; all three could be effective to various degrees and could function in different arenas and at different institutional levels — international, national, community, and family.
The Commission followed the third path for some of the reasons outlined above. Nevertheless, because it appears that human rights are given a diminished role in Path 3 in comparison to the first two paths, it seems worthwhile to examine the intellectual and strategic motivations for pursuing each of the different ways of engaging with human rights to advance health and health equity.
On seeing the lack of medical supplies in Malawi as part of the causal chain of maternal mortality among poor women, Farmer was motivated to ask the questions in terms of “should there be a right?” because there are in fact, no enunciated human rights to sutures, to sterile drapes, or anesthesia. If there were indeed such human rights to sutures and other relevant medical supplies and services stated in the law, the concern would, understandably, be about enforcement and implementation of the legal rights. Indeed, a significant part — if not most — of the health and human rights scholarship over the past decade has concerned interpreting, implementing, or enforcing the right to health and other human rights related to health already existing in international law. But there is no such explicitly articulated legal right to sutures. Nevertheless, Farmer continues to press this example in terms of human rights law, calling attention to a broader definition of human rights that encompasses economic and social rights. Although no explicit human right to sutures is stated in either the Universal Declaration of Human Rights, the Covenant on Economic, Social and Cultural Rights, or in Right to Health General Comment No. 14, the existing language and rights in these legal human rights documents can be interpreted to provide individuals with a right to such essential health care supplies as sutures, sterile drapes, and anesthesia. Should effectively realizing this interpretation prove difficult, then it may still be possible to interpret rights to these supplies in the more recent conventions and declarations. For those who are disturbed about the unjustifiable lack of life-saving materials — that is, of medical neglect — such a search to make use of human rights law is motivated by both the fact that economic and social rights are intended to guarantee the material needs of human beings, and because human rights law is law; it has potential power — legal, political, and moral — to make governments and, increasingly, other actors, behave in particular ways to provide material goods and social conditions.
Farmer presents an additional line of reasoning for increased enforcement of economic and social rights (that is, pursuing Path 1), aside from the fact that they imply rights to various health care goods and services. He argues that more vigorous enforcement of economic and social rights would improve living conditions, leading to better health outcomes. To carry this point further, such improved health achievements would, in turn, also create more active citizens and democratic institutions. At the risk of being too simplistic, the reasoning for pursuing Path 1 would be to argue that where the causes of preventable morbidity and mortality are due to medical neglect and material privation, the enforcement of economic and social rights will provide health care, create conditions for better health and longevity, and create stronger social and political institutions. Farmer and many other individuals following this line of reasoning exhort practitioners of health and human rights and public health communities (and anyone else with the power to effect change) to fight against the entrenched orthodoxies in so many arenas, and to champion the enforcement and realization of economic and social rights. From this perspective, it is understandable, then, why human rights advocates express disappointment when analysis of health issues, especially on a global scale, is not explicitly framed in terms of existing human rights law, particularly an overarching right to health. It appears to be a wasted opportunity, one that fails both to recognize and make use of the entitlements identified in human rights law at the same time it fails to help support the efforts for greater enforcement and implementation of human rights law, particularly economic and social rights.
It is on this point — the recognition of the effects of economic and social conditions on the health of individuals and populations — that social medicine and human rights perspectives converge. The practice of social medicine has a long history and its practitioners have been centrally focused on the social conditions affecting the health of the worst off in societies. There has always been an overlap between those who are socially excluded from economic, political, and other resources and those who bear the highest burden of poor health. The causal relationship between poor health and social, economic, and political deprivations would understandably lead any medical professional working with the socially excluded to draw on concepts of protections and entitlements such as those enshrined in international human rights. Where it is clearly visible that the social structure — the social, economic, and political conditions and underlying ideologies — is allowing or, indeed, directly causing avoidable disease and deaths on a large scale, the idea and law of human rights appears to be the only available mechanism to fight back; one might envision human rights in such a setting acting as a safety net that empowers those who suffer most egregiously to claw back up the great chasm of inequality and deprivation. Moreover, in the present era of increasing globalization, international human rights law may be the best available instrument to address the ill health caused by transnational actors who are, in many cases, more powerful than some governments.
Before presenting points seen as critical of such rights-based approaches to health issues — especially as these paths reflect the perspectives of individuals whom we greatly admire — it seems appropriate and necessary to recall the words of Onora O’Neill, a notable philosopher who has written extensively on human rights. When asked by one of the authors of this article why she seems to be so critical of some arguments for human rights while also being so emphatically concerned with acute deprivations in the world, she replied that it is because we care so much about the idea of human rights that we must ensure that arguments to support them are unimpeachable.19 So, it is our hope that our evaluation of the first two approaches — increased enforcement of economic and social rights (Path 1) and infusing principles of human rights legislation into health programs and interactions between individuals on the ground (Path 2) — should not be misunderstood as being critical of the idea of human rights in our effort to share our reasoning for choosing the third path, which appears to diminish the role of human rights in comparison to the first two. It is indeed because we care about the idea of human rights greatly that we are publicly presenting our reasoning. Sofia Gruskin, Editor of this journal for over a decade, expressed a similar concern when she wrote that “[g]reater clarity about the central paradigms of health and human rights is essential to make our work more effective, as well as to enable us to make counter-arguments that will be persuasive not only to the skeptics but to the public health community at large.”20
This idea that international human rights law taken as a whole offers both rights to health care and rights to the social and material conditions for good health was argued by Jonathan Mann and colleagues in the very first issue of this journal in 1994.21 Central to their “health and human rights framework” hypothesis was the notion that “the promotion and protection of human rights and promotion and protection of health are fundamentally linked.”22 It was evidently clear in the early 1990s, in light of the way HIV/AIDS was being dealt with in most countries, that public health programs can negatively affect human rights and that human rights violations can have negative health effects. Mann and colleagues transformed the conflict between a public health policy perspective and a human rights perspective into a hypothesis that a society that realizes the full breadth of human rights would produce healthier individuals and populations. Health programs, they argued, whether public health or clinical, that were in line with human rights would lead to better health outcomes, and the respect for all human rights would create conditions for individuals to be healthier. In fact it should be noted that the Commission has expressed a similar view in the Final Report that correctly designing the social processes in society to meet the needs or expand freedoms of its members will improve health and health equity. The Commission was able, rather than presenting it as a hypothesis, to make this argument as a conclusion drawn from empirical research.
One remarkable aspect of Mann’s 1994 hypothesis is that it leads to conceptualizing human rights law as one component of a model of causation and distribution of health. This is illustrated in the discussion about possible ways to test the hypothesis, where Mann and his colleagues wrote, “For example, health professionals could consider using the International Bill of Human Rights as a coherent guide for assessing health status of individuals or populations; the extent to which human rights are realized may represent a better and more comprehensive index of well-being than traditional health status indicators.”23 While it was a groundbreaking contribution to overlay human rights law onto an analysis of the causes, distribution, and social responses to health issues, the consequent substitution of human rights law for the actual causes of ill health in a model of causation and distribution of health is problematic. As evident in our sutures example, for instance, the distinction between the lack of sutures and the lack of the right to sutures in explaining maternal mortality is profound in many respects and should not be minimized.
The observation that the lack of sutures plays a role in the causes of maternal mortality necessarily precedes reasoning that there should be a right to sutures. This epistemological priority or precedence of recognizing the causal role of the lack of sutures to the assertion that there should be a right to sutures is the source of consequent divergence between a social epidemiology/social medicine and a human rights approach to advancing health and health equity. Some human rights advocates would likely want to assert that it is the violation of the right to sutures that causes maternal mortality. When it is asserted that the lack of a right to something is the cause of ill health and mortality, the distinction between the causal role and importance of that something and the right to that something collapses. Moreover, the collapsing of the two ideas creates confusion as to what is a human right. Human rights are not natural facts or objects, but ethical assertions about claims, privileges, liberties, immunities, and powers in relation to various human capabilities, including those capabilities expressed indirectly via material things.24 Unnecessary and avoidable misunderstandings result from attempting to emphasize the importance of human rights by casting them as direct causal components of a model of causation and distribution of ill health and mortality. Moreover, such attempts undermine the important scientific analysis of causal pathways and distribution of ill health and open the analysis to the risk of being dismissed as conceptually incoherent. Last, such an analysis potentially alienates social and natural science researchers who can be valuable allies in the effort to advance health equity. The health and human rights framework can be very powerful indeed, if it supplements rather than attempts to substitute the analysis of the natural and social causes, distribution, and consequences of ill health and mortality. We suggest further below one possible way that epidemiology and human rights might be integrated.
But what about the case in which someone is advocating a right to sutures after recognizing the lack of sutures as a direct cause of maternal mortality? For the practitioner of social medicine, the primary aim is not to enforce economic and social rights, or any other rights, for their own sake. Rather, the preeminent goal is to address avoidable ill health and mortality, the curtailment of well-being. Therefore, enforcement of economic and social rights is instrumental in order to address the needs for health care and other social conditions and material goods. The problem arises when the law is silent about some pressing concern, or when the law is insufficient, or, indeed, incoherent. Aside from being entangled in legal rubric, stretching the law to cover the causes, cures, and other necessary social interventions for some particular health deprivation may begin to look like “the tail is wagging the dog.” When there is no right to sutures, and yet the lack of sutures leads to the deaths of hundreds of thousands of women each year, it is understandable to seek a right to sutures somewhere in the law. Yet neither the existing economic and social rights nor any language in the current human rights corpus may be capable of doing all the work we want them to do. At the same time, it would be unacceptable to conclude that the causes that are killing people are not human rights concerns simply because they are not explicitly identified in the existing law, and also unacceptable to opportunistically stretch the meaning of rights so much that the term “human rights” risks becoming an empty concept. Indeed, it is very helpful if some human rights exist in the law that have direct bearing on a health issue at hand, but human rights law should be recognized as being only one of many instruments of advancing health and health equity.
The second problem with following Path 1 — increased enforcement of economic and social rights — is one of insufficient motivating capacity. The large number of human rights advocacy organizations in the world testifies to the fact that the mere existence of human rights law does not mean that human rights are universally or even locally realized. Even at the domestic level, laws identifying certain rights do not mean that individuals, especially those that are socially marginalized, have their rights respected or fulfilled. To exhort that the full spectrum of legal rights must be respected because it says so in the law requires a respect for law, the means to enforce it, and mechanisms to hold individuals or institutions accountable for violations. While motivating respect for rights is difficult and requires constant vigilance and resources, it is nearly impossible to enforce a right to something that may not clearly exist in the law, especially in places where there is no respect for the law or a lack of institutions to enforce rights. It should not go unnoticed, however, that individuals and communities throughout the world recognize and respect various rights even when such rights are not specifically stated in the law. And if they are in the law, respecting such rights may not be primarily motivated by the fact they are enshrined in the law. Before the relatively recent establishment of international human rights law, advocates for the respect of human rights and for social change drew on arguments for why such things are good and “the right thing to do.” Public statements to provide such reasoning were often accompanied by large-scale social mobilization; indeed, this ethico-moral approach was often much more comprehensive than the method currently employed by rights activists, of pointing to what is explicitly stated in the law and playing language games. Realizing rights, whether economic and social or civil and political, by means of assertions that they must be respected simply because it says so in international law, is neither necessary nor sufficient for advancing health and health equity — unless and until international law has the power to command full adherence and there are institutional capacities and resources in all countries to (progressively) realize all human rights.
In an attempt partially to overcome many of the structural and conceptual problems in engaging with human rights law, Lynn Freedman has proposed an alternative approach to expand the reach and relevance of human rights “on the ground.”25 Her strategy is innovative in that it seeks to supplement the dominant approach to human rights work that takes place within international institutions as academic and legal discussions, and instead focuses on holding governments accountable for upholding human rights. We suggest Freedman’s approach as our Path 2. Freedman advocates a strategy that extracts various values and principles from existing human rights law and applies them to local contexts — the on-the-ground analysis of the causal chain of ill health and mortality. While Freedman focuses on addressing maternal mortality, and her approach fits nicely with our example of the right to sutures, this strategy could be applied to addressing any health issue.
Motivated by the understanding that human dignity is the core value of human rights law and is meant to inspire profound and fundamental change in everyday interactions, Freedman proposes communities identify a set of values and principles in human rights law and then articulate how they can help guide community-level programs to address maternal mortality. Using the case of the right to sutures, following Freedman’s path would mean that we do not look for a right to sutures in the law but that the values and principles of human rights law can help communities identify, analyze, and address maternal mortality. In fact, Freedman interprets the legal discourse on the human right to health as encompassing the right not to die an avoidable death in pregnancy and childbirth. This right then translates into a societal obligation to provide emergency obstetric care, which would entail the provision of sutures when needed. But even when dealing with nongovernmental actors and a concern not just about sutures but maternal mortality more broadly, Freedman argues that the two values of human dignity and non-discrimination (among others), which are central to human rights law, can and should guide the manner in which emergency obstetric care is provided to patients and families as well as how it impacts hospital staff. This strategy may be seen as expanding human rights work, perhaps even liberating human rights from the existing legal language and mechanisms of international law. Importantly, rather than making rights into causal components of health and well-being, Freedman suggests that human rights values and principles, when combined with other health-related disciplines such as epidemiology, medicine, and operations research, can provide a plan of action for communities and states — in other words, human rights discourse can become a community health planning tool.
Although it is an important and worthwhile strategy to apply human rights law to the reality of how individuals are living their daily lives, this path also suffers from insufficient power as a tool for motivation. It is unclear as to why the values and principles that Freedman uses to guide maternal mortality programs should be convincing to others simply on the basis of their presence in human rights legislation. Indeed, is it not ethical reasoning that first produced the values that then became enshrined as various rights in human rights law? That is, why would individuals and communities change their views and behaviors from the status quo to be in line with these values because these values are derived from human rights law? Granted, there is an international consensus embodied in such laws, but how convincing is it that individuals need to work and interact or programs are designed and operated in accordance with certain values and principles because they were derived from human rights law? Perhaps more persuasive would be an ethical or moral argument. Why not present these values and principles as being important in the analysis of health issues and require allegiance because it is the right thing to do, or is what is demanded by social justice? Dignity, non-discrimination, equality, and participation are all values than can be highlighted within the ethical reasoning concerning what to do about maternal mortality in communities throughout the world. Synthesizing scientific and empirical insights from fields such as epidemiology, medicine, operations research, and public health with ethical reasoning about social justice by communities should be just as motivating — if not more so — for taking action than arguing that certain value-motivated actions are required simply because the values can be found in human rights law.
Path 2, as argued by Freedman, is indeed the middle ground between Path 1 and Path 3 (the path taken by the Commission). The first path, in its best form, seeks to link the causal and distributional analysis of health issues with international human rights law. The second path seeks to craft and guide a social response by integrating various values with necessary and helpful insights from different fields while remaining grounded in human rights law. The third path can be seen as being a step farther away from either of the first two, as it seeks to derive values from ethical reasoning that takes place at community-level, national, regional, and global spheres. The initial conclusion of that ethical reasoning, which took place within the Commission and is now ongoing and open to all, was to classify ill health and health inequalities that are avoidable through reasonable means as inequities. Furthermore, the Commission determined that such manifest inequities must be addressed as a matter of social justice. In addition to this ethical argument — that if one can reasonably prevent ill health and death, one should do so — is the argument that one must act to address social determinants of ill health and health inequalities on the basis of the duties to protect, promote, and fulfill relevant human rights.
There is broad convergence between research and action on rights-based approaches and social determinants of health when existing international agreements about human rights encompass actions to address the relevant social determinants. Indeed, perhaps it can be argued that enunciated rights and values implicit in human rights law cover the entire gamut of the social determinants of ill health and mortality. However, social epidemiology has more explanatory potential than human rights approaches because the objects of research are not themselves ethical assertions, nor is the scope of social epidemiology limited by what is written in the law. Yet human rights law has the power to bridge social epidemiology with social action. The power of human rights lies in its prescriptive power to guide prospective social action through identifying legal obligations as well as underlying moral obligations of societies to act in particular ways. However, local and global discussions that link social epidemiological analysis with ethical reasoning about social justice would involve more actors and allow for a broader scope of social action, more expansive rights and responsibilities, and easier social acceptance. It is necessary to find a way to integrate these two approaches.
Perhaps one method that avoids the conflation of causal factors and human rights is to incorporate rights as distal factors in the chain of causation. A social environment that does not protect, promote, or fulfill the rights to food, clothing, shelter, or civil and political liberties can be understood to have a role in the chain of causation and distribution of ill health without being a direct causal factor. It would also make understandable the assertion that if individuals have a right to health, then they should also have a right to the determinants of health. In this way, integrating epidemiology and human rights — or constitutional rights for that matter — would illuminate the role of the lack of rights in the causal chain of ill health and mortality, while also avoiding having to show that every violation of a human right is bad for health. Such an integrated framework could move forward the agenda to improve health and health equity by harnessing the power of both human rights and epidemiology.
Joint projects for the future
Given that social epidemiology, social medicine, and human rights-based approaches are all important and productive methodologies to advance health and health equity, it behooves all involved to attempt to build greater inter-theoretic coherence and collaboration. There is undoubtedly much to be gained intellectually and practically from interdisciplinary efforts. We suggest four possible areas for action with an open invitation for further proposals.
First, there is the obvious need to undertake a more thorough mapping of the Commission’s existing analysis using human rights law. This is not to explain ill health and inequalities in terms of human rights violations, but rather to identify what is required in the form of social action as a matter of law. It may also be worthwhile to investigate how to motivate social action at the community level to address the social determinants of ill health and health inequalities through enriching local deliberations with human rights principles. Second, much could be gained from bringing together social epidemiology and human rights analyses to develop policy indicators for the implementation of the Commission’s recommendations as well as progressive realization of the right to health. Third, the Commission has (hopefully) achieved one of its main goals, to bring equity to the center of discussions on health. Human rights advocates could help considerably by providing support in the form of human rights-based arguments for addressing social gradients in health. Last, not least important, a rights-based approach to health causes, distribution, and consequences must be created, one that is informed by, and builds inter-theoretic coherence with, social epidemiology as well as other relevant fields, not least of which are public health, economics, and operations research.
Acknowledgments
The authors would like to thank the editors and reviewers for their valuable assistance. Research for the article was made supported by the Joint ESRC–DFID Scheme for research on international poverty reduction (RES–167–25–0369) and the Department of Health in England.
Sridhar Venkatapuram MSc, MPhil, PhD, is the ESRC–DFID Research Fellow in the Department of Epidemiology and Public Health and a member of the Centre for Philosophy, Justice and Health, at University College London, United Kingdom.
Ruth Bell, PhD, is a Senior Research Fellow in the Department of Epidemiology and Public Health at University College London.
Michael Marmot, MPH, PhD, FRCP, FFPHM, FMedSci, is Head of the Department of Epidemiology and Public Health, University College London, and served as Chairman of the WHO Commission on Social Determinants of Health and the Strategic Review of Health Inequalities in England Post 2010. He is currently Chair of the European Review on the social determinants of health and the health divide.
Please address correspondence to the authors c/o Sridhar Venkatapuram, UCL Department of Epidemiology and Public Health, 1–19 Torrington Place, London WC1E 6BT, United Kingdom, email: s.venkatapuram@ucl.ac.uk.
References
1. Information about the Commission is available at http://www.who.int/social_determinants/thecommission/en/index.html. For the complete final report, see Commission on Social Determinants of Health, Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health (Geneva: World Health Organization, 2008). Available at http://whqlibdoc.who.int/publications/2008/9789241563703_eng.pdf.
2. Ibid.
3. The three principles of action are listed in Commission on Social Determinants of Health (see note 1), p. 2.
4. World Health Organization, “WHA 62.14: Reducing health inequities through action on the social determinants of health,” in World Health Organization, Sixty-second World Health Assembly, Geneva, 18–22 May 2008, resolutions and decisions, annexes (Geneva: World Health Organization, 2009), pp. 21–24. Available at http://apps.who.int/gb/ebwha/pdf_files/WHA62-REC1/WHA62_REC1-en.pdf.
5. World Health Organization, World Health Statistics 2009 (Geneva: World Health Organization, 2009).
6. P. Farmer, “Challenging orthodoxies: The road ahead for health and human rights,” Health and Human Rights: An International Journal 10/1 (2008), pp. 5–19; the discussion on sutures, sterile drapes, and anesthesia is at p. 9. Available at http://www.hhrjournal.org/index.php/hhr/article/view/33/102.
7. Commission on Social Determinants of Health (see note 1), p. 3.
8. M. Murphy, M. Bobak, A. Nicholson, et al., “The widening gap in mortality by educational level in the Russian Federation, 1980–2001,” American Journal of Public Health 96/7 (2006), pp. 1293–1299.
9. M. Tobias, T. Blakely, D. Matheson, et al., “Changing trends in indigenous inequalities in mortality: Lessons from New Zealand,” International Journal of Epidemiology 38/6 (2009), pp. 1711–1722.
10. R. Fang, A. Kmetic, J. Millar, and L. Drasic, “Disparities in chronic disease among Canada’s low-income populations,” Preventing Chronic Disease 6/4 (2009), pp. 1–9. Available at http://www.cdc.gov/pcd/issues/2009/oct/08_0254.htm.
11. O. Lundberg, M. Å. Yngwe, M. K. Stjärne, et al., The Nordic experience: Welfare states and public health (NEWS), Health Equity Studies 12 (Stockholm: Centre for Health Equity Studies [CHESS], Stockholm University/Karolinska Institutet, 2008). Available at http://www.chess.su.se/content/1/c6/02/90/15/NEWS_Rapport_080819.pdf.
12. On this point, see discussion in Commission on Social Determinants of Health (see note 1), pp. 32–33.
13. M. Marmot, “Health in an unequal world,” Lancet 368/9552 (2006), pp 2081–2094.
14. Commission on Social Determinants of Health, (see note 1), p. 63.
15. A. Sen, Development as freedom (New York: Knopf, 1999); M. Marmot, Status syndrome: How your social standing directly affects your health and life expectancy (London: Bloomsbury, 2004).
16. P. Hunt, “Missed opportunities: Human rights and the Commission on Social Determinants of Health,” Global Health Promotion 1757-9759 (2009), Supp 1, pp. 36–41, doi: 10.1177/1757975909103747. Available at http://physiciansforhumanrights.org/students/right-to-health-ghac/missed-opportunities.pdf.
17. Farmer (see note 6), p. 9.
18. Ibid.
19. Personal communication.
20. S. Gruskin, “Rights-based approaches to health: Something for everyone” [Editorial], Health and Human Rights: An International Journal 9/2 (2006), p. 6. Available at http://www.hhrjournal.org/archives-pdf/4065399.pdf.bannered.pdf.
21. J. Mann, L. Goskin, S. Gruskin, et al., “Health and human rights,” Health and Human Rights: An International Journal 1/1 (1994), pp. 6–23. Available at http://www.hhrjournal.org/archives-pdf/4065260.pdf.bannered.pdf.
22. Ibid., p. 21.
23. Ibid.
24. A. Sen, The idea of justice (London: Allen Lane, 2009); J. J. Thomson, The realm of rights (Cambridge, MA: Harvard University Press, 1990).
25. L. P. Freedman, “Using human rights in maternal mortality programs: From analysis to strategy,” International Journal of Gynecology and Obstetrics 75 (2001), pp. 51–60.