Emmanuel Kabengele Mpinga, Henk Verloo, Leslie London, and Philippe Chastonay
Health and Human Rights 13/2
Published December 2011
Abstract
Background
Over the past decades, the health and human rights movement has become a public health actor that cannot and should not be ignored when defining public health policies. Little has been published about the scientific contribution of the movement, be it in terms of volume, topics, content, diffusion channels, production, or target sites.
Objective
This article aims to characterize the scientific production of articles focusing on “health and human rights” and to describe its evolution over a decade.
Methods
A systematic review of the literature was done. The following databases were considered: Medline, Embase, BDSP, Wholis, Saphir, Rero and Web of Science. The analysis focused on English and French contributions published between January 1, 1999 and December 31, 2008.
Results
Nine hundred twenty eight articles, published in 377 different journals, were reviewed. Among these articles, 43.7% had been written by one author and 56.3% by two or more authors. Over the studied decade, the production volume increased threefold. Most frequent developed topics were related to health systems (18.3%), mental health (11.5%), HIV/AIDS (10.3%), reproductive health (9.2%). Emerging topics included: the rights of patients (2.7%), new technologies (2.5%), and handicap (2.5%). Studies were classified according to their design in social analysis (42.7%), reviews of the literature (19.8%), qualitative studies (17.9%), editorials (12.5%), epidemiological studies (6.8%).
Most studies were published in public health (34.5%) and biomedical journals (29.0%), while some appeared in social science journals (4.7%). The studies were related to global issues/settings (43.9%) or more specifically to country settings, for example, the United States (9.3%), Great Britain (7.8%), South Africa (3.3%), Australia (3.0%), Canada (2.6%), France (2.3%), and India (1.9%). The authors were mainly from industrialized countries.
Conclusion
The publication of articles on health and human rights issues is increasing, and new topics are being addressed. Yet more evidence-based studies might be necessary to scientifically strengthen the domain.
Background
The health and human rights movement has grown with the expansion of the HIV/AIDS pandemic and has experienced many developments over the past decade.1 In the academic field, notable changes include the development of health and human rights training programs, especially in medical and public health schools; the creation of specific professorships at universities; the addition of scientific journals focusing on health and human rights; and international conferences.2 At the United Nations level, many developments took place, such as the normative interpretation of the right to health in 2000 by the Committee on Social, Economic and Cultural Rights; the nomination of the Special UN Rapporteur on the Right to Health in 2002; the creation at WHO of a unit on health and human rights; and the adoption by the UN General Assembly of the Millennium Declaration.3 Other developments took place, notably at the global health governance level, but also at state levels, with the initiation of health care reforms including more equity and solidarity of the social insurance systems, ultimately strengthening the links between achieving health and the respect of basic human rights.4 More recently, the health and human rights movement has also addressed issues related to pandemics, climate change, and famines.5
On the normative level, the human rights protection mechanisms have been strengthened by the adoption and ratification of various international treaties, such as the Convention on the Rights of Persons with Disabilities (2006), Optional Protocols to the Convention against Torture (2009), and the International Convenant on Social, Economic and Cultural Rights (2009). The South African Treatment Action Campaign, centered on the access to HIV tritherapies, illustrates these developments.6 On a more technical level, research on appropriate indicators monitoring the right to health has been a crucial contribution.7
Little is known about the scientific production that occurred in response to those developments. Two reviews give some insight, however. In 2000, Flanagin published a review on publications focusing on human rights that appeared in the biomedical literature between 1966 and 1999.8 The author’s conclusion pointed to the responsibility of medical journals to support publications in the field of human rights, especially when related to health. Furthermore, in 2005, Jimba et al reviewed articles on health and human rights that were published in Japanese medical journals between 1983 and 2002, and saw an increase of published articles over the studied period.9 We are not aware of any other reviews trying to characterize the scientific production of articles on health and human rights.
Such studies are useful to scientists involved in human rights advocacy, to political decision-makers in the evaluation of public health policies, and to teachers of human rights training programs. Such studies allow us to discover patterns in the structure of scientific fields, identify processes of knowledge dissemination, and visualize the dynamics of scientific developments. In the context of new research areas such as health and human rights, such studies are necessary in order to obtain an overall view of intellectual structure of a field, to consider scientific impact, or to suggest how a field might move forward.10
The aim of our study is less ambitious. Its objective is to characterize, in terms of content, topics, authorship, and geographic distribution, the scientific production on health and human rights that has been published over the past decade, and to contribute to a better understanding of this field and to its development.
Methods
Data
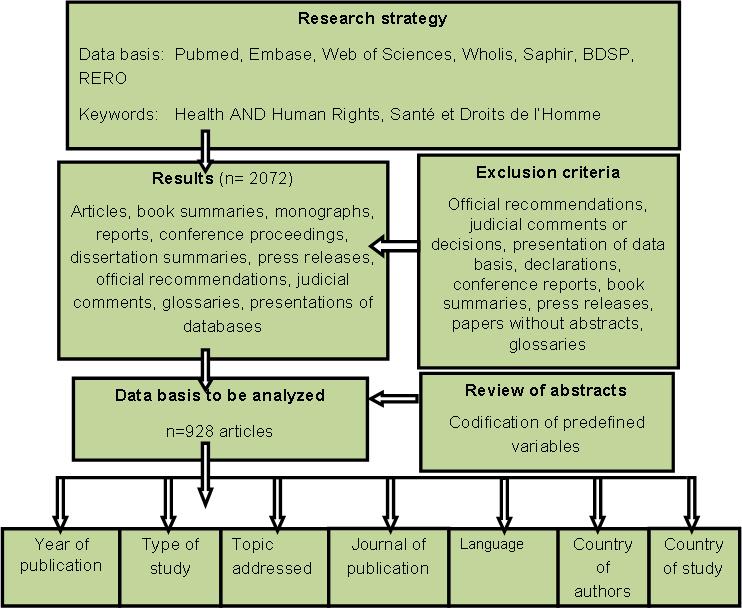
A systematic review of the French and English literature was undertaken, targeting the period of January 1, 1999 to December 31, 2008. The following databases were explored: Medline, Embase, BDSP, Wholis, Saphir, Rero and Web of Science. The investigated keywords were “health and human rights” in English and “santé et droits de l’homme” or “santé et droits humains” in French. The research strategy focused on the Mesh descriptors associated with the keywords human rights, human rights abuses, health, health status disparities, delivery of health care, health policy, public health, health services accessibility, état de santé, santé publique, accès aux soins, inégalités de soins, droits fondamentaux. The adopted research strategy and number of references obtained from each database are presented in Annex 1.
Exclusion criteria
A first selection identified 2,072 references. After excluding papers without an abstract, official recommendations, judicial comments or decisions, declarations, conferences proceedings, books reviews, press releases, and glossaries, a final list of 928 articles was available for analysis. Where there were differences of opinion regarding the status of the item (n=22), these were allocated through discussion within the team and were finally included into the studied set.
Analyzing procedure
Two of the authors (EKM, HV) independently checked each article for the following items, which were then listed in an Excel database (as a reading frame): Year of publication, type of journal, study design, research topic, country of origin of authors, country setting of the study, and language. The year of publication was identified based on the reference in the abstract. For each abstract, the journal in which the article was published was identified and classified according to a pre-established categorization, for example: biomedical journals (for example, World Psychiatry, PLoS Med), journals of epidemiology or public health (for example, Global Public Health, J Epidemiol Community Health), journals of health care (for example, Issues Ment Health Nurs). Regarding study design, four categories were defined (editorials, qualitative studies, epidemiological studies, social analysis and reviews) according to established categorization.11 The study design was defined and codified according to this categorization.
Regarding research topics, we adopted the approach of Fluss and Amnesty International, published in 1999 in Health and Human Rights, in identifying the major topic as described in the abstract.12 Each article’s country of origin was identified through the affiliation address of the first author for the Medline articles. For articles mentioned in the other databases, the authors used Find Articles and Google Scholar. The authors affiliated with an international organization were put into the category of “international organization.” The country of study was determined through information in the abstract. Each country was attributed a specific code and the studies done in a specific country were assigned this specific country code.
Studies done at supranational levels with a mention of the region were attributed to the mentioned region (for example, Europe); when two continents were involved, studies were assigned to the category “multi-site.” Publications with a focus on moral, ethical, and philosophical dimensions were assigned to the category “global issues.” Two authors (EK and HV) encoded the various studies independently. Differences of encoding were resolved through discussion. A consensus-based database was eventually constructed. The fourth author (PC) reviewed the Excel database for potential encoding errors. The data was then exported to IBM-SPSS 19.0 for descriptive analysis.
Figure 1. Methodology of the research strategy
Results
The results, summarized in Tables 1 to 5, are based on 928 articles reviewed and published from 1999 to 2008 in French or English; the articles appeared in 377 journals, with a mean of 2.26 articles per journal over the 10-year period. The number of journals having published at least one article on health and human rights rose from 28 journals in the first year to 72 in the last year. More than a third of the articles (35.23%) were published in a set of 20 journals with a stable mean over the period considered (Table 1).
Table 1. Twenty journals with most articles on health and human rights over the 10-year period 1998-2008
| Journal | 2008 | 2007 -2000 | 1999 | TOTAL | % |
| 1. Reprod Health Matters | 8 | 25 | – | 33 | 3.56% |
| 2. Am J Public Health | 4 | 20 | 8 | 32 | 3.45% |
| 3. Med Law | 6 | 15 | 8 | 29 | 3.13% |
| 4. Health Hum Rights | – | 21 | 4 | 25 | 2.69% |
| 5. Lancet | 4 | 21 | 0 | 25 | 2.69% |
| 6. Soc Sci Med | 2 | 17 | 1 | 20 | 2.16% |
| 7. Med Confl Surviv | 5 | 9 | – | 14 | 1.51% |
| 8. Int J Gynaecol Obstet | – | 12 | 2 | 14 | 1.51% |
| 9. Can HIV AIDS Policy Law Newsl | – | 12 | 1 | 13 | 1.40% |
| 10. J Med Ethics | – | 13 | – | 13 | 1.40% |
| 11. Acta Psychiatrica Scandinavica | – | 12 | – | 12 | 1.29% |
|
12. Bull World Health Organ |
1 | 11 | – | 12 | 1.29% |
| 13. JAMA | – | 10 | 2 | 12 | 1.29% |
| 14. HIV AIDS Policy Law Rev | 1 | 10 | – | 11 | 1.19% |
| 15. J Epidemiol Community Health | 1 | 9 | 1 | 11 | 1.19% |
| 16. J Law Med | 8 | 3 | – | 11 | 1.19% |
| 17. Public Health | 2 | 9 | – | 11 | 1.19% |
| 18. Dev World Bioeth | 4 | 6 | – | 10 | 1.08% |
| 19. Int J Health Serv | – | 8 | 2 | 10 | 1.08% |
| 20. S Afr Med J | 2 | 7 | – | 9 | 0.97% |
| Total | 48 | 250 | 29 | 327 | 35.23% |
Around 43% of the published studies are social analyses. Qualitative studies make up 17.9%, while epidemiologic studies represent 6.8%, and reviews 19.8%. Twelve and a half percent are editorials. (Table 2).
Table 2. Types of health and human rights studies reported
| Designs | n | % |
| 1. Editorials | 116 | 12.5 |
| 2. Qualitative studies | 166 | 17.9 |
| Descriptive studies without survey | 63 | 6.8 |
| Case studies | 58 | 6.3 |
| Qualitative studies with precise design | 45 | 4.8 |
| 3. Epidemiologic studies | 64 | 6.8 |
| Descriptive quantitative studies | 56 | 6.0 |
| Cohort studies | 4 | 0.4 |
| Case-control studies | 4 | 0.4 |
| 3. Social analyses | 397 | 42.7 |
| Sociopolitical analyses | 155 | 16.7 |
| Ethic/moral analyses | 105 | 11.3 |
| Legal and medico-legal analyses | 89 | 9.6 |
| Historical studies | 34 | 3.7 |
| Philosophical analyses | 5 | 0.5 |
| Economic studies | 5 | 0.5 |
| Theological analyses | 2 | 0.2 |
| Anthropological studies | 2 | 0.2 |
| 4. Reviews | 184 | 19.8 |
| Simple review | 174 | 19.3 |
| Systematic reviews | 4 | 0.4 |
|
Meta-analyses |
1 | 0.1 |
| Total |
928 |
100.0 |
Research domains are numerous and diverse, yet a vast majority (77.6%) of the publications are related to ten topics: health systems (18.3%), mental health (11.5%), HIV/AIDS (10.3%), reproductive health (9.2%), health and human rights in general (7.7%), violence (6.8%), health and migration (4.6%), research in medicine and public health (3.1%), the rights of children (3.1%), and issues in ethics (3.0%). New topics also appear, such as the rights of patients, new technologies, handicap, health and trade, and health of minorities (Table 3).
Table 3. Classical and new research themes in the field of health and human rights
| Classical Themes |
n |
% |
New Themes |
n |
% |
| Health systems |
170 |
18.3 |
Right of patients |
25 |
2.7 |
|
Mental health |
107 |
11.5 |
New technologies |
23 |
2.5 |
| HIV/AIDS |
96 |
10.3 |
Handicaps |
23 |
2.5 |
| Reproductive health |
85 |
9.2 |
Right to health |
19 |
2.0 |
| Health and Human rights |
71 |
7.7 |
Health and trade |
17 |
1.8 |
| Violence |
63 |
6.8 |
HHR training |
14 |
1.5 |
| Health and migration |
43 |
4.6 |
Humanitarian crisis |
11 |
1.2 |
| Medical/public health research |
29 |
3.1 |
HHR and environment |
10 |
1.1 |
| Right of children |
29 |
3.1 |
HHR of minorities |
9 |
1.0 |
| Issues in ethics |
28 |
3.0 |
Right to food |
9 |
1.0 |
| Others* |
47 |
5.0 |
|||
| Subtotal |
721 |
77.6 |
207 |
22.3 |
|
| Total |
928 |
100.0 |
*Among others:
Torture (0.6%), international cooperation (0.5%), elderly people (0.4%), palliative care (0.4), death penalty (0.2), right to housing (0.2%), health and sports (0.1%)
In Table 4, we list the types of journals that published the articles. Most articles (74.9%) were published in biomedical and public health journals. Around 20% were published in “mixed” journals (for example, medicine and law, medicine and social sciences), whereas less than 1% was published in journals dealing specifically with law. Regarding language, 95.4% of the papers were in English.
Table 4. Categories of journals
| Journals |
n |
% |
| 1. Biomedical and care journals |
373 |
40.1 |
| Biomedicine |
266 |
29.0 |
| Nursing |
34 |
4.0 |
| Ethics and bioethics |
68 |
7.0 |
| Medical technologies |
5 |
0.1 |
| 2. Journals of public health |
323 |
34.8 |
| Epidemiology and public health |
320 |
34.5 |
| Health economics |
3 |
0.3 |
| 3. Mixed journals |
188 |
20.2 |
| Medicine and law |
95 |
10.2 |
| Medicine and social sciences |
62 |
6.7 |
| Health and human rights |
31 |
3.3 |
| 4. Journals of social sciences |
44 |
4.7 |
| Political sciences |
33 |
3.6 |
| Law |
7 |
0.7 |
| Human rights |
3 |
0.3 |
|
Finance |
1 |
0.1 |
|
Total |
928 |
100.0 |
Table 5 shows the countries of authors’ residence and the country in which each study took place. The most common countries of authors’ residence were the United States (30.4%), Great Britain (18.0%), Canada (8.7%), Australia (7.3%), South Africa (4.6%), France (3. 3%), India (2. 4%), Brazil (2.7%) and Switzerland (1.6%).
Table 5. Study settings and authorship countries
| Authorship Countries |
n |
% |
Study Settings |
n |
% |
| USA |
282 |
30.4 |
Global issues |
407 |
43.9 |
| United Kingdom |
167 |
18.0 |
USA |
86 |
9.3 |
| Canada |
81 |
8.7 |
United Kingdom |
72 |
7.8 |
| Australia |
68 |
7.3 |
South Africa |
31 |
3.3 |
| South Africa |
43 |
4.6 |
Europe (as a region) |
31 |
3.3 |
| France |
31 |
3.3 |
Australia |
28 |
3.0 |
| India |
22 |
2.4 |
Canada |
24 |
2.6 |
| Brazil |
21 |
2.3 |
Multi-site (two continents) |
21 |
2.3 |
| Switzerland |
15 |
1.6 |
France |
21 |
2.3 |
| International organizations |
24 |
2.6 |
India |
18 |
1.9 |
| Others |
174 |
18.7 |
Others |
189 |
20.3 |
| Total |
928 |
100.0 |
Total |
928 |
100.0 |
The country settings in which most studies took place are the United States (9.3%), Great Britain (7.8%), South Africa (3.3%), Australia (3%), Canada (2.6%), France (2.3%) and India (1.3%). Of note is the number of studies done in a global setting or perspective (43.9%) or at a regional level (Europe 3.3%, multi-site 2.3%).
Discussion
The scientific production in the field of health and human rights has shown an important increase over the time period studied. This is in accordance with previous observations by Flanagin, who reported 2,096 papers listed on Medline between 1966 and 1990 versus 9,000 between 1995 and 1999.8 Jimba et al reported a similar trend in 2005.9 The reasons for this evolution might be related to the increasing interest of health and human rights for health professionals, or even for the scientific community at large. This increasing interest could be related to new evidence, such as the relationship between poverty and the HIV/AIDS epidemic. It could also be a trend as it becomes more politically correct to show an interest in the field. By analogy, one might mention the sharp increase of scientific articles on new developments such as the electronic individual medical record (11 papers in 1992 versus 256 in 2005).13 One might also mention the explosion of epidemiologic studies over the past 25 years, as reported, for example, by Barreto (a twelvefold increase).14
The increase of published articles on health and human rights over the years may be attributable to new journals entering the field, or to existing journals allotting more space to health and human rights. It could also be related to new paradigms appearing with emerging disciplines.15 With the emergence of the health and human rights movement, conceptual clarification of the initial paradigm was implemented. Indeed, at present the links between rights and health are well accepted, as are the links with social and political implications.
In our review, a majority of the studies are social analyses; only a few studies have primary empirical data. Recently, The Journal of Human Rights Practice published a special issue that tackles the scientific evidence in the field of health and human rights, arguing that there are too few evidence-based studies.16 This is not singular to health and human rights. Borry et al recently reported that between 1990 and 2003, only 435 out of 4,029 bioethics articles (10.8%) corresponded to true evidence-based study designs.17 One might regret the few economic, historical, philosophical, or theological studies, which could have brought some new perspectives to a field that must be rooted in several disciplines.
In assessing our research strategy, the crucial question is the extent to which the investigated journals and studies represent the overall situation. The research strategy was centered on keywords, which seemed more reliable and better standardized than an approach centered on thematic areas (for example, violence against women, access to health care, contraception, or quality of care).
Though many of the studies in our review focus on traditional health and human rights topics such as health systems, mental health, or HIV/AIDS, new topics often appear; for example, health and human rights in relation with new technologies, environmental issues, humanitarian crises. Flanagin reported five main topics: ethics, torture, international health, public health, and refugees. Jimba et al indicated that while mental health was the main topic between 1983 and 1987, patients’ rights later became the main topic.8.9
With new technologies and resulting social change come new ethical considerations that may require new legislation addressing economic and commercial issues (for example, patentability) and moral challenges (for example, euthanasia). Such legislation may impair basic human rights; these topics belong in the corpus of health and human rights publications.
A bibliometric study limited to Medline on the scientific production in bioethics in Spain (852 documents) between 1966 and 2003 indicates that genetics and cloning publications accounted for 0% between 1966 and 1983, 6.1% between 1984 and 1993, and 13.8% between 1994 and 2003. Terminal illness publications accounted for 6.4% during the first period and 14.4% during the last.18 This evolution may be due in part to scholars’ increasing interest in topics being debated at the legislative or societal levels, thus contributing to the justification or refusal of either party’s arguments. UNESCO’s Declaration of Human Genome and Human Rights and the European Convention on Human Rights and Bio-Medicine, both adopted in 1997, are examples of legislation that may have stimulated the interest and scientific production of health and human rights scholars.
Most of the studies in our review were published in biomedical or public health journals. Publication habits vary from one scientific field to another: it is essential for scholars in biomedical sciences to publish articles; while in social sciences and law, scholars tend to publish books.19 Our review underestimates the contribution of books to health and human rights, because we excluded book reviews from our study. Furthermore, neither chapters of books nor communications at conferences have been integrated into our analysis.
The geographic distribution of the studied publications shows that the overwhelming majority are published in developed countries. There is an emphasis on local or national problems, yet an interest in global issues. Seventy percent of the authors in our review are residents of industrialized nations. Recent bibliometric studies have reported similar observations. Paraje et al, while studying scientific publications from the health sector between 1992 and 2001, reported that more than 90% of those publications were produced in as few as 20 countries.20 Soteriades and Falagas analyzed 48,861 articles published between 1995 and 2003 on preventive medicine, occupational and environmental medicine, epidemiology, and public health, and found that 93.4% of the publications were based in the United States, Canada, Western Europe, Japan, and Australia. African and Latin American authors contributed to 2.3% of the publications.21
Several factors might explain these facts; funding is certainly one. In 2003, according to the Global Forum for health research, 92% of the research done in the health sector had been funded by the G7 member states.22 Indeed, very little money is invested into research in developing countries. But other factors have also been mentioned, such as the role of states in organizing research, as well as the development of human resources and the counter-lobbying of some international institutions.23
Considering the geographic distribution of the articles, we see evidence of a few trends emerging: in Brazil, several studies investigate access to health care for people living with HIV. In Australia, several studies focus on the right to health of the migrant population. If indeed there was such a trend, it is conceivable that we will begin to see regions emerging as centers of specific competencies.
Our review focused on French and English publications; more than 90% of those studied were written in English. There is an important selection bias: Spanish-language publications were not included. Additional representative data on “language and scientific publication,” such as the Paraje et al study in 2005 highlights the dominance of the English language: out of 3.47 million scientific publications edited in 4,061 scientific journals from 190 countries and in 23 languages, 96% are in English.20
Though done according to established procedures, our review has limitations.24 Researching via keywords has possibly led to the exclusion of specific journals which do not systematically use keywords. This might explain, for example, the non-representation of articles published in BMC International Health and Human Rights, a leader in the field, but one which does not use keywords (the journal is represented only by six papers where automatic search functions generated keywords). One might also argue that the bibliographic research should have focused on common topics in the field of health and human rights. Such an approach might have covered the field more thoroughly, but very difficult to implement due to the number of topics that should have been addressed. Some authors have tried such an approach, selecting a finite number of topics related to health and human rights.12 This approach still leaves other topic areas uncovered, however. In our review, which included information from seven databases, an approach with 15 to 20 specific topics would have been too difficult to implement. Our study might not be exhaustive, yet our observations are quite real (increase of scientific production, appearance of new topics, and the predominance of certain study designs).
There are, without doubt, publications that are not listed in the consulted databases. Our method of article selection may also have missed articles from other regions, such as Eastern Europe or Southeast Asia, since researchers in these areas tend to publish their findings in regional journals more than researchers in other regions tend to do.25 It is, of course, difficult to measure the potential contribution of those studies to new knowledge in the field of health and human rights.
Besides keywords and abstracts, no other bibliometric elements, such as the citation index, have been studied. The citation index, for example, might have given some insight into the impact of certain studies and on the existing networks among researchers.
Our study was limited to articles written in English and French. Therefore, we missed work published in other languages, such as Spanish, Japanese, or German. This might have affected our results, even though many groups from these areas publish in English, and even though the importance of scientific publications in those languages has diminished over the years; Bordons and Gomez showed this decrease in their study on the Web Science Publication Index: the percentage of scientific publications in these languages was 6.5% in 1980, 3.4% in 1990, and 1.7% in 2000.26
Research perspectives and recommendations
Our study is a first attempt to characterize and analyze this area of research. While it has certain limitations, it could also set the standard for further studies in this field, which could contribute to better understanding and promote this area.
More points could have been investigated, such as the production by author, by teams, by institution or even by networks, which could have yielded interesting new information on health and human rights. Such research could enrich the debate and perhaps promote the implementation of a specific international agenda on health and human rights.
The wide range of journals publishing health and human rights articles may be a positive sign. The number of journals focusing solely on health and human rights, however, is small (two out of the 377 studied). There seems to be an interest in promoting the development of new journals in the field, perhaps especially at regional levels publishing local and regional studies.
In our view, some lessons can be learned. There seems to be a need to:
- reinforce centers with specific competencies in education and training, in advocacy and lobbying, in political governance on HHR;
- stimulate the emergence of regional and international research networks and contribute to the creation of new scientific or community-oriented journals;
- clarify the epistemology status of “health and human rights.” The question does not seem to have been defined, discussed, or solved, and thus far, the scientific production in the field has not produced a coherent theoretical effort allowing definition of the field’s limits, its founding principles, or its dominant currents;
- strengthen the evidence base for research, which would consolidate the link between health and human rights and give it more force at the judicial and advocacy levels;
- develop training programs oriented towards high-risk domains such as life sciences, or high risk groups such as health professionals;
- demonstrate the impact of produced knowledge on health policies and practices, or on human rights protection strategies;
- promote and support research initiatives in developing countries, where human rights violations are prevalent and health problems generalized;
- support the constitution of professionals involved in research, promotion, advocacy, and interventions in health and human rights; and
- develop a health and human rights knowledge database.
Conclusion
This literature review aims to analyze the scientific publications in the field of health and human rights, to define its characteristics, and to measure its evolution. Our review of the literature produced on health and human rights gives some insight into the relevant research trends over the past decade, as well as into challenges the field is facing.
Though most publications appeared in public health and biomedical journals, our results underline the constant evolution of the scientific production in this field, showing that new topics were investigated over the years. Our study also shows the very small amount of studies originating in developing countries, though health and human rights conditions are critical in many of these countries.
In our view, it would be worthwhile to further consolidate the health and human rights field in promoting quality research. This would allow to establish more scientific evidence and to take public health decision based on sound scientific data. Based on our observations, there appears to be a need to promote publication of health and human rights studies in interdisciplinary journals (notably, law and medicine). Further, there are challenges related to the epistemological nature of the concept “health and human rights.”
All this calls for the scientific community to show more interest in investigating the field, and for the political decision makers to consider it when developing health strategies. The health and human rights movement will have to face these challenges in order to appear as an autonomous and multidisciplinary actor of prime importance for the health of the population.
Acknowledgements
The authors thank the staff of the Centre de documentation en santé publique du CHUV for their help in defining and implementing the research strategy.
Emmanuel Kabengele Mpinga, MHA, MPH, PhD, is Associate Professor SSPH+ of Health and Human Rights, at the Institute of Social and Preventive Medicine, Department of Community Health and Medicine, Faculty of Medicine, University of Geneva, Geneva, Switzerland.
Henk Verloo, RN, MSc, PhD candidate, is Professor at Applied University of Health Sciences La Source, Lausanne, Switzerland.
Leslie London, MD, MSc, MMed, is Professor at the School of Public Health & Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa.
Philippe Chastonay, MD, MPH, is Associate Professor of Public Health at the Institute of Social and Preventive Medicine and the Unit of Development and Research in Medical Education, Faculty of Medicine, University of Geneva, Geneva, Switzerland.
Please address correspondence to Professor Emmanuel Kabengele Mpinga, IMSP-CMU, Michel Servet 1, 12 11 Geneva 4, Geneva, Switzerland; email: Emmanuel.Kabengele@unige.ch.
References
1. S. Gruskin, J.D. Mills, and D. Tarantola, “Health and human rights 1: History, principles and practice of health and human rights,” Lancet 370 (2007), pp. 449-455.
2. J. Brenner, “Human rights education in public health graduate schools: A survey,” Health and Human Rights: An International Journal 2/1 (1996), pp. 129-139; E.L. Cotter, J. Chevrier et al, “Health and human rights education in US schools of medicine and public health: Current status and future challenges,” Plos ONE 4/3 (2009), p. e4916; Health and Human Rights: An International Journal and BMC Int Health and Human Rights; Human Rights Conferences Worldwide. Available at http://www.conferencealerts.com/humanrights.htm.
3. United Nations Economic and Social Council. The right to the highest attainable standard of health. General Comment 11/08/2000. E/C.12/2000/4, Geneva, May 2000; United Nations Commission of Human Rights. Res 2002/31, Geneva, April 2002; United Nations General Assembly. Resolution A/Res/55/2 of September 13th in relation with the Millennium Declaration. New York, September 2000; D. Tarantola, “A perspective on the history of health and human rights: from the cold war to the gold war,” Journal of Public Health Policy 29/1 (2008), pp. 42-53.
4. E. Docteur and H. Oxley, Health care systems: Lessons from the reform experience. OECD Health Working Paper 9, Paris 2003, p. 97; H. Maarse, “The privatization of health care in Europe: An eight country analysis,” Journal of Health Politics, Policy, and Law 31/5 (2006), pp. 981-1014; X. Liu and A. Mills, “Financing reforms of public health services in China: lessons for others nations,” Soc Sci Med 54/11 (2002), pp. 1691-1698; P.G. Marchildon, “Canadian health system reforms: lessons for Australia?” Austr Health Rev 29/1 (2005), pp. 105-119; A. Sekwat, “Health financing reform in Sub-Saharan: major constraints, goals, and strategies,” J Health Care Finance 29/3 (2003), pp. 67-78; E.K. Mpinga and P. Chastonay, “Health and human rights: Perceptions of health professionals and human rights defenders,” Santé Publique 17/3 (2005), pp. 371-383.
5. C.K.B. Choi and A.W.P. Pak, “Lessons for surveillance in 21 century: A historical perspective from past five millennia,” Soz and Prev Med 6/46 (2001), pp. 361-368; J.A. Patz, T. Campbell-Lendrum, and T. Holloway, “Impact of regional climate change on human health,” Nature 438 (2005), pp. 3110-3111; H.J. Brinkman, S. de Pee, I. Sanogo et al, “High food prices and the global financial crisis have reduced access to nutritious food and worsened nutritional status and health,” The Journal of Nutrition 2009 doi: 10.3945/jn.109.110767; M. Heywood, “Drug access, patents and global health: chaffed and waxed sufficient,” Third World Quarterly 23/2 (2002), pp. 217-231.
6. M. Heywood, “South Africa’s treatment action campaign: Combining law and social mobilization to realize the right to health,” Journal of Human Rights Practice 1/1 (2009), pp. 14-36.
7. G. Backman, P. Hunt, R. Khosla et al. “Health systems and the right to health: An assessment of 194 countries.” Lancet 372 (2008), pp. 2047-2085.
8. A. Flanagin, “Human rights in biomedical literature: The social responsibility of medical journals,” JAMA 284/5 (2000), pp. 618-619.
9. M. Jimba, Y. Nomura, C.K. Poudel et al,“Increase of health and human rights research articles in Japan,” JMAJ 48/11 (2005), pp. 545-549.
10. F.J. Van Raan Anthony, “The use of bibliometric analysis in research performance assessment and monitoring of interdisciplinary scientific developments,” Technikfolgenabschatzung 1/12 (2003), pp. 20-29; F.G.A. De Bakker, P. Groenewegen, and F. Den Hond, “A bibliometric analysis and theory on corporate social responsibility and corporate social performance,” Business Society 2005; 44/3(2005), pp. 283-316.
11. W. Ahrens and I. Pigeot, Handbook of Epidemiology (Birkhauser, Bremen) 2005, p. 1617; C.D. Miller and N.J. Salkin, Handbook of Research Design and social measurement (Sage Publications. Thousand Oaks, London, New Delhi) 6th edition, 2002, 786p.
12. S.S. Fluss, “A select bibliography on Health and Human Rights 1984-1999,” Health and Human Rights 1999; 4/1(1999), pp. 265-276; Amnesty International, “Publications on Health and Human Rights Themes 1982-1998,” Health and Human Rights 1999; 4/1(1999): 215-264.
13. W. Hysien-Chia, Yuh-Shan et al, “Scientific production of electronic health record research, 1991-2005,” Computer Methods and Programs in Biomedicine 86/2 (2007), pp.191-196.
14. M.L. Barreto, “Growth and trends in scientific production in epidemiology in Brazil,” Rev Saude Publica 40 (2006), pp. 79-85.
15. A. Michalopoulos, M.E. Falagas, “A bibliometric analysis of global research production in respiratory medicine,” CHEST 128 (2005), pp. 3993-3998; M. Aragona, “A bibliometric analysis of the current status of psychiatric classification: The DSM model compared to the spectrum and dimension diagnosis,” Giorn Ital Psicopat 12 (2006), pp. 342-351.
16. R. Archer, “Introduction to the special issue: Where is the evidence?” Journal of Human Rights Practice 1 (2009), pp. 333-338.
17. P. Borry, P. Schostman et al, “Empirical research in bioethical journals: A quantitative analysis,” J Med Ethics 32 (2006), pp. 240-245.
18. I. Belinchon, J.M. Ramos, and V. Beliver, “Scientific production in bioethics in Spain through Medline,” Gac Sanit 21/5 (2007), pp. 408-411.
19. A.J. Nederhof, “Bibliometric monitoring of research in the social sciences and humanities: A review,” Scientometrics 66/1 (2006), pp. 81-100.
20. G. Paraje, R. Sadan et al, “Increasing international gaps in health-related publications,” Science 308/5724 (2005), pp. 959-960.
21. S.E. Soteriades and E.M. Falagas, “A bibliometric analysis in the fields of preventive medicine, occupational and environmental medicine, epidemiology and public health,” BMC Public Health 6 (2006).
22. Global Forum for Health Research, “Monitoring financial flows for health research.” Report 2006, p. 105.
23. A.M. Lansang and R Dennis, “Building capacity research in developing world,” Bulletin of the World Health Organization 82 (2004), pp. 764-770; F. Salager-Meyer, “ Scientific publishing in developing countries: Challenges for the future,” Journal of English Academic Purposes 7 (2008), pp. 121-132.
24. H.J. Littell, J. Corcoran, and V. Pillai, Systematic Reviews and Meta-analysis (New York: Oxford University Press), 2008; A. Liberati, D.G. Altman, J. Tetzlaff et al, “The Prisma Statement of Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Health care interventions: Explanation and Elaboration,” PLoS Med 6/7 (2009), p. e1000100.
25. P.I. Vergidis, A.I. Karavasiou, K. Paraschakis, I.A. Blioziotis, and M.E. Falagas, “Bibliometric analysis of global trends for research productivity in microbiology,” Eur Journ Microbiol Infect Dis 24 (2005), pp. 342-345.
26. M. Bordons and I. Gomez, “Towards a single language in science? A Spanish view,” Serials 17/2 (2004), pp. 189-195.
Annex 1. Details of search strategy (in French and English)
| Database | Keywords | Mesh | Parameters and Results |
| 1. Medline | Human rightsHuman rights abusesHealthHealth statusHealth policyDelivery of care | Human rights,Human rights abusesHealth, Men’s health, Mental health,Minority health, Public healthWomen’s health, World HealthHealth status, Health status disparityHealth PolicyDelivery of care,
Health service accessibility Health services disparties |
1 Human Rights/ (4618)2 Human Rights Abuses/ (267) 3 1 or 2 (4841) 4 health/ or men’s health/ or mental health/ or minority health/ or public health/ or women’s health/ or world health/ (60863) 5 health status/ or health status disparities/ (32104) 6 “delivery of health care”/ or health services accessibility/ or healthcare disparities/ (47526) 7 Health Policy/ (22418) 8 5 or 6 or 4 or 7 (147427) 9 3 and 8 (1436) 10 limit 9 to (yr=”1999 – 2008″ and (english or french)) (1087) 11 health.m_titl. (140538) 12 human rights.m_titl. (1140) 13 11 and 12 (296) 14 limit 13 to (yr=”1999 – 2008” and (english or french)) (238) 15 10 or 14 : 1172 references |
| 2. Embase | Human rightsHuman rights abusesHealth | Human rightsHuman rights abusesHealth, Minority health, Public healthWomen’s health, World HealthHealth status, Health status,Health care policy, Health disparityHealth care delivery, Health care disparity | ((‘human rights’/mj OR ‘human rights abuse’/mj OR ‘human rights’:ti OR ‘human rights’:ab) AND (‘health’/de OR ‘mental health’/de OR ‘men`s health’/de OR ‘minority health’/de OR ‘public health’/de OR ‘women`s health’/de OR ‘health status’/de OR ‘health disparity’/de OR ‘health care delivery’/de OR ‘health care disparity’/de OR ‘health care policy’/de)) OR (health:ti AND ‘human rights’:ti) AND ([english]/lim OR [french]/lim) AND [embase]/lim AND [1999-2008]/py: Results: 710 references |
| 3. BDSP | SantéDroits homme | Santé, Etat de santé, Santé mentaleSanté publique, Accès aux soinsInégalités aux soins, Politique de santéDroits fondamentaux, Droits de l’hommeAtteintes aux droits de l’hommeDroits humains | Recherche à l’aide des mots clés (descripteurs) BDSP: mcl=”droits fondamentaux” AND (mcl=”etat sante” OR mcl=”sante mentale” OR mcl=”sante publique*” OR mcl=”acces soins” OR mcl=”inegalite devant soins” OR mcl=”politique sante”) AND (date=2008 OR date=2007 OR date=2006 OR date=2005 OR date=2004 OR date=2003 OR date=2002 OR date=2001 OR date=2000 OR date=1999)212 référencesOU Recherche au titre : Santé et droits de l’homme / Santé et droits humains ((titdoc=sante AND titdoc=droit*) AND (titdoc=humain* OR titdoc=homme)) AND (date=2008 OR date=2007 OR date=2006 OR date=2005 OR date=2004 OR date=2003 OR date=2002 OR date=2001 OR date=2000 OR date=1999)26 référencesOU Recherche au titre : Health and Human Rights (titdoc=health AND titdoc=human AND titdoc=right*) AND (date=2008 OR date=2007 OR date=2006 OR date=2005 OR date=2004 OR date=2003 OR date=2002 OR date=2001 OR date=2000 OR date=1999) 51 référencesTotal (après exclusion des doublons) 252 référence |
| 4. WHOLIS | HealthHuman rights | Health and all others Mesh mentioned aboveHuman rightsHuman rights abuses | Subject “human rights” AND subject “health” [AND language = French and publication year =1999-2008]: 11 referencessubject “human rights” AND subject “health” [AND language = English and publication year =1999-2008] :52 références: 1 référence non retenue (en espagnol)La recherche par descripteur est complétée ensuite par une recherche par mots du titre : Santé et droits de l’homme OU Santé et droits humains OU Health and Human Rightstitle “droits homme” AND title “sante” search found 2 titlestitle “droits humains” AND title “sante” search found 4 titles.title “human rights” AND title “health” search found 25 titlesRésultat (après exclusion des doublons) 67 références |
| 4. SAPHIR | HealthHuman rights | Health and all others Mesh mentioned aboveHuman rights, Human rights abuses | Recherche par descripteurs élargie à tous les thésaurusMesh, BDSP, CORAS et ISPALa recherche par descripteur est complétée ensuite par une recherche par mots du titre Santé et droits de l’homme 13 références ; OU Santé et droits humains 7 références OU Health and Human Rights, 5 référencesRésultat total (après exclusion des doublons): 23 Références |
| 5. RERO | HealthHuman Rights | Health and all others Mesh mentioned aboveHuman rights, Human rights abuses | Santé et droits de l’homme OU Partout: sante et droits humains OU Partout: Health and Human Rights 1999-2008: 87 notices; Résultat : 87 Références |
| 6. Web of science | Health AND Human Rights | Title= (health) AND Title= (human rights)Refined by: Languages= (ENGLISH OR FRENCH); Timespan=1999-2008; Results: 256 References | |
| Summing up after exclusion of duplicates | MEDLINE: 1,169EMBASE: 496BDSP: 209WHOLIS: 61SAPHIR: 23RERO: 18Web of Science 96 TOTAL: 2,072 |
Annex 2. Journals publishing studied articles
| Journal | Number of Articles on HHR | % of Total Articles on HHR |
| Acad Emerg Med | 1 | 0.11% |
| Account Res | 1 | 0.11% |
| Acta Clin Croat | 1 | 0.11% |
| Acta Paediatr | 1 | 0.11% |
| Acta Psychiatrica Scandinavica Suppl | 12 | 1.29% |
| Acta Sociologica | 1 | 0.11% |
| Actualité et Dossier en Santé Publique | 2 | 0.22% |
| Actualités Sociales Hebdomadaires | 1 | 0.11% |
| Afr J AIDS Res | 1 | 0.11% |
| Age and Aging | 1 | 0.11% |
| AIDS | 6 | 0.65% |
| AIDS Care | 2 | 0.22% |
| AIDS Care Psychol Socio-Med Asp AIDS HIV | 3 | 0.32% |
| AIDS public policy | 1 | 0.11% |
| AIDS Reader | 2 | 0.22% |
| Alter | 1 | 0.11% |
| Am J Bioeth | 1 | 0.11% |
| Am J Crit Care | 1 | 0.11% |
| Am J Forensic Psychiatry | 1 | 0.11% |
| Am J Ind Med | 1 | 0.11% |
| Am J Ment Retard | 1 | 0.11% |
| Am J Nurs | 1 | 0.11% |
| Am J Orthopsychiatry | 4 | 0.43% |
| Am J Prev Med | 1 | 0.11% |
| Am J Public Health | 32 | 3.45% |
| Ambul Pediatr | 1 | 0.11% |
| American Anthropologist | 1 | 0.11% |
| Anil Aggrawal’s Internet J Forensic Med Toxicol | 1 | 0.11% |
| Ann Health Law | 1 | 0.11% |
| Ann Intern Med | 1 | 0.11% |
| Ann New York Acad Sci | 3 | 0.32% |
| Ann Surg | 1 | 0.11% |
| Annales Médico-Psychologiques | 1 | 0.11% |
| Annu Rev Public Health | 3 | 0.32% |
| Annual Review of Anthropology | 1 | 0.11% |
| ANS Adv Nurs Sci | 3 | 0.32% |
| Anthropol Med | 1 | 0.11% |
| Arch Dis Child | 2 | 0.22% |
| Arch Ophthalmol | 1 | 0.11% |
| Arch Pediatr | 1 | 0.11% |
| Arch Pediatr Adolesc Med | 1 | 0.11% |
| Arch Sex Behav | 4 | 0.43% |
| Asia Pac J Public Health | 1 | 0.11% |
| Asian Journal of Wto & International Health Law and Policy | 1 | 0.11% |
| Aust J Prim Health | 1 | 0.11% |
| Aust N Z J Public Health | 7 | 0.75% |
| Aust New Zealand J Psychiatry | 1 | 0.11% |
| Aust Nurs J | 1 | 0.11% |
| Australas Psychiatry | 5 | 0.54% |
| Behav Sci Law | 1 | 0.11% |
| Best Pract Res Clin Obstet Gynaecol | 7 | 0.75% |
| Bioethics | 7 | 0.75% |
| BMC Int Health Hum Rights | 6 | 0.65% |
| BMC Med | 2 | 0.22% |
| BMC med ethics | 1 | 0.11% |
| BMC Public Health | 4 | 0.43% |
| Br J Clin Gov | 1 | 0.11% |
| Br J Fam Plann | 1 | 0.11% |
| Br J Nurs | 1 | 0.11% |
| Br J Occup Ther | 1 | 0.11% |
| Br J Psychiatry | 4 | 0.43% |
| Br J Psychother | 1 | 0.11% |
| Br Med J | 5 | 0.54% |
| Br. Med bull | 2 | 0.22% |
| Brain Inj | 1 | 0.11% |
| Bull Med Ethics | 1 | 0.11% |
| Bull World Health Organ | 12 | 1.40% |
| Bulletin Juridique De La Santé Publique | 3 | 0.32% |
| Cad Saude Publica | 1 | 0.11% |
| Cahier Pratique Tissot | 1 | 0.11% |
| Cahiers De La Puéricultrice | 1 | 0.11% |
| Cahiers Psychiatriques | 2 | 0.22% |
| Camb Q Healthc Ethics | 1 | 0.11% |
| Cambridge Quarterly of Healthcare Ethics | 1 | 0.11% |
| Can Fam Phys | 1 | 0.11% |
| Can HIV AIDS Policy Law Newsl | 13 | 1.40% |
| Can J Psychiatry | 2 | 0.22% |
| Can J Public Health | 6 | 0.65% |
| Cancer | 1 | 0.11% |
| Cand Nurse | 1 | 0.11% |
| Child Abuse Negl | 1 | 0.11% |
| Child Adolesc Psychiatr Clin North Am | 1 | 0.11% |
| Child Care Health Dev | 1 | 0.11% |
| Child Welfare | 1 | 0.11% |
| Chronobiol Int | 1 | 0.11% |
| Clin Med | 1 | 0.11% |
| Clin Med J R Coll Phys Lond | 1 | 0.11% |
| Clin Oral Investig | 1 | 0.11% |
| Clin Perinatol | 1 | 0.11% |
| Clin Pharmacol Ther | 1 | 0.11% |
| Clin Psychol | 1 | 0.11% |
| Clin Psychol Sci Pract | 1 | 0.11% |
| Clinical Child Psychology and Psychiatry | 1 | 0.11% |
| CMAJ | 1 | 0.11% |
| Common Law World Rev | 1 | 0.11% |
| Commun Dis Public Health | 1 | 0.11% |
| Community Genet | 1 | 0.11% |
| Community Pract | 1 | 0.11% |
| Cornell Law Rev | 1 | 0.11% |
| Cost Eff Resour Allocat | 1 | 0.11% |
| Crit Pub Health | 3 | 0.32% |
| Croat Med J | 6 | 0.65% |
| Cult Health Sex | 2 | 0.22% |
| Curationis | 2 | 0.22% |
| Curr Opin Psychiatry | 3 | 0.32% |
| Curr Paediatr | 1 | 0.11% |
| Curr Probl Pediatr Adolesc Health Care | 1 | 0.11% |
| Dev World Bioeth | 10 | 1.08% |
| Diabetes Care | 1 | 0.11% |
| Dig Dis | 1 | 0.11% |
| Disabil Rehabil | 2 | 0.22% |
| Disability & Society | 1 | 0.11% |
| Disasters | 3 | 0.32% |
| Dossiers D’Etudes – CAF | 1 | 0.11% |
| Drug Alcohol Rev | 1 | 0.11% |
| Drug Dev Res | 1 | 0.11% |
| East Mediterr Health | 1 | 0.11% |
|
ENSP |
1 | 0.11% |
| Environ Health Perspect | 1 | 0.11% |
| Environ Sci Technol | 1 | 0.11% |
| Epidemiology | 1 | 0.11% |
|
Eth Human Psychol Psychiatry |
1 | 0.11% |
| Eth Human Sci Services | 1 | 0.11% |
| Ethn Health | 3 | 0.32% |
| Eur Hum Rights Law Rev | 1 | 0.11% |
| Eur J Cancer Care (Engl) | 1 | 0.11% |
| Eur J Epidemiol | 1 | 0.11% |
| Eur J Health Law | 9 | 0.97% |
| Eur J Public Health | 4 | 0.43% |
| Fraternitaire | 1 | 0.11% |
| Gac Med Mex | 1 | 0.11% |
| Gen Hosp Psychiatry | 1 | 0.11% |
| Gender Med | 1 | 0.11% |
| Gerontologist | 1 | 0.11% |
| Global Public Health | 5 | 0.54% |
| Globalization Health | 3 | 0.32% |
| Gynecol Obstet Fertil | 1 | 0.11% |
| Harm Reduct J | 1 | 0.11% |
| Hastings Cent Rep | 1 | 0.11% |
| Health Aff (Millwood ) | 1 | 0.11% |
| Health Care Anal | 6 | 0.65% |
| Health Care Anal | 1 | 0.11% |
| Health Care Women Int | 1 | 0.11% |
| Health Econ | 1 | 0.11% |
| Health Econ Policy Law | 1 | 0.11% |
| Health Educ Res | 1 | 0.11% |
| Health Hum Rights | 25 | 2.69% |
| Health Place | 1 | 0.11% |
| Health Policy | 4 | 0.43% |
| Health Popul Perspect Issues | 1 | 0.11% |
| Health Promot Int | 1 | 0.11% |
| Health Promot J Austr | 1 | 0.11% |
| Health Soc Work | 1 | 0.11% |
| Heroin Addict Relat Clin Probl | 1 | 0.11% |
| HIV AIDS Policy Law Rev | 11 | 1.19% |
| HIV AIDS Rev | 1 | 0.11% |
| HIV Med | 1 | 0.11% |
| Hum Fertil (Camb) |
1 |
0.11% |
| Hum Reprod |
1 |
0.11% |
| Human Rights Quarterly |
2 |
0.22% |
| Indian J Med Ethics |
4 |
0.43% |
| Indian J Med Res |
2 |
0.22% |
| Indian J Pract Pediatr |
1 |
0.11% |
| Int Clin Psychopharmacol |
1 |
0.11% |
| Int J Cosmet Surg Aesthet Dermatol |
1 |
0.11% |
| Int J Dermatol |
1 |
0.11% |
| Int J Disabil Hum |
1 |
0.11% |
| Int J Drug Policy |
8 |
0.86% |
| Int J Environ Health Res |
1 |
0.11% |
| Int J Equity Health |
1 |
0.11% |
| Int J Gynaecol Obstet |
14 |
1.51% |
| Int J Health Serv |
10 |
1.08% |
| Int J Inj Contr Saf Promot |
1 |
0.11% |
| Int J Law Psychiatry |
4 |
0.43% |
| Int J Law Psychiatry |
1 |
0.11% |
| Int J Ment Health Syst |
1 |
0.11% |
| Int J Occup Environ Health |
6 |
0.65% |
| Int J Prison Health |
4 |
0.43% |
| Int J Psychiatr Nurs Res |
1 |
0.11% |
| Int J STD aids |
1 |
0.11% |
| Int J Tuberc Lung Dis |
1 |
0.11% |
| Int. rev. Psychiatry |
6 |
0.65% |
| Intern Med J |
3 |
0.32% |
| Ir J Psychol Med |
3 |
0.32% |
| Issues Ment Health Nurs |
1 |
0.11% |
| J Acquired Immune Defic Syndr |
1 |
0.11% |
| J Adolesc Health |
1 |
0.11% |
| J Adv Nurs |
1 |
0.11% |
| J Am Coll Dent |
1 |
0.11% |
| J Am Dent Assoc |
1 |
0.11% |
| J Am Med Womens Assoc |
3 |
0.32% |
| J Ambul Care Manage |
4 |
0.43% |
| J Appl Philos |
2 |
0.22% |
| J Biolaw Bus |
1 |
0.11% |
| J Biosoc Sci |
2 |
0.22% |
| J Can Dent Assoc |
1 |
0.11% |
| J Child Adolesc Ment Health |
1 |
0.11% |
| J Child Health Care |
1 |
0.11% |
| J Chin Med Assoc |
1 |
0.11% |
| J Clin Psychol |
1 |
0.11% |
| J Coll Phys Surg Pak |
1 |
0.11% |
| J Cult Divers |
1 |
0.11% |
| J Cyst Fibrosis |
1 |
0.11% |
| J Dent Educ |
2 |
0.22% |
| J Emerg Prim Health Care |
1 |
0.11% |
| J Epidemiol Community Health |
11 |
1.19% |
| J Forensic Med Toxicol |
1 |
0.11% |
| J Forensic Psychiatry Psychol |
1 |
0.11% |
| J Health Commun |
1 |
0.11% |
| J Health Hum Serv Adm |
1 |
0.11% |
| J Health Law |
2 |
0.22% |
| J Health Popul Nutr |
1 |
0.11% |
| J Health Psychol |
1 |
0.11% |
| J Health Serv Res Policy |
1 |
0.11% |
| J Health Soc Policy |
1 |
0.11% |
| J Homosex |
1 |
0.11% |
| J Hum Nutr Diet |
1 |
0.11% |
| J Immigr Minor Health |
1 |
0.11% |
| J Indian Med Assoc |
3 |
0.32% |
| J Int Bioethique |
4 |
0.43% |
| J Intellect Disabl |
7 |
0.75% |
| J Interprof Care |
2 |
0.22% |
| J Law Med |
11 |
1.19% |
| J Law Med Ethics |
8 |
0.86% |
| J Med Ethics |
13 |
1.40% |
| J Med Leg Droit Med |
1 |
0.11% |
| J Med Liban |
1 |
0.11% |
| J Med Philos |
3 |
0.32% |
| J Ment Health |
5 |
0.54% |
| J Midwifery Womens Health |
2 |
0.22% |
| J Miss State Med Assoc |
1 |
0.11% |
| J Nerv Ment Dis |
1 |
0.11% |
| J Obstet Gynecol Neonatal Nurs |
1 |
0.11% |
| J Paediatr Child Health |
1 |
0.11% |
| J Pain Symptom Manage |
1 |
0.11% |
| J Public Health (Germany) |
1 |
0.11% |
| J Public Health (Oxf) |
1 |
0.11% |
| J Public Health Med |
1 |
0.11% |
| J Public Health Policy |
5 |
0.54% |
| J R Soc Med |
1 |
0.11% |
| J R Soc Promot Health |
1 |
0.11% |
| J Sex Marital Ther |
1 |
0.11% |
| J Sex Res |
1 |
0.11% |
| J Trauma Stress |
2 |
0.22% |
| J Trop Pediatr |
1 |
0.11% |
| J Vasc Nurs |
1 |
0.11% |
| J Vocat Rehabil |
1 |
0.11% |
| J Women’s Health |
2 |
0.22% |
| JAMA |
12 |
1.29% |
| Japan Med Assoc J |
3 |
0.32% |
| JET – Le Bulletin D’Epiter |
1 |
0.11% |
| JMS J Med Soc |
1 |
0.11% |
| Journal International De Bioéthique et éthique |
1 |
0.11% |
| Journal Of Substance Abuse Treatment |
1 |
0.11% |
| Kennedy Inst Ethics J |
2 |
0.22% |
| Lancet |
25 |
2.69% |
| Lancet Neurol |
1 |
0.11% |
| Law Hum Behav |
1 |
0.11% |
| Le Journal De La Démocratie Sanitaire |
1 |
0.11% |
| Lepr Rev |
2 |
0.22% |
| Les Cahiers Français |
1 |
0.11% |
| Leukemia |
1 |
0.11% |
| L’Infirmière Du Québec |
1 |
0.11% |
| L’Information Psychiatrique |
1 |
0.11% |
| McGill Law J |
1 |
0.11% |
| Med Confl Surviv |
14 |
1.51% |
| Med Glas |
1 |
0.11% |
| Med J Aust |
5 |
0.54% |
| Med J Malaysia |
1 |
0.11% |
| Med Law |
29 |
3.13% |
| Med Law Int |
6 |
0.65% |
| Med Sci Law |
1 |
0.11% |
| Med Sci Monit |
1 |
0.11% |
| MedGenMed |
1 |
0.11% |
| Medgenmed Medscape Gen Med |
1 |
0.11% |
| Ment Health Reforms |
3 |
0.32% |
| Metab Brain Dis |
1 |
0.11% |
| Metaphilosophy |
1 |
0.11% |
| Midwifery |
3 |
0.32% |
| Monash Bioeth Rev |
1 |
0.11% |
| N Z Bioeth J |
1 |
0.11% |
| Nat Immunol |
1 |
0.11% |
| Nat Rev Gen |
1 |
0.11% |
| Natl Med J India |
1 |
0.11% |
| Nature |
1 |
0.11% |
| Neurourol Urodyn |
1 |
0.11% |
| New Genet Soc |
1 |
0.11% |
| New Zealand Med J |
1 |
0.11% |
| Nicotine Tob Res |
1 |
0.11% |
| Nurs Clin North Am |
3 |
0.32% |
| Nurs Ethics |
5 |
0.54% |
| Nurs Forum |
1 |
0.11% |
| Nurs Health Sci |
2 |
0.22% |
| Nurs Inq |
1 |
0.11% |
| Obstet Gynecol Surv |
1 |
0.11% |
| Occup Med (Lond) |
1 |
0.11% |
| Online J Issues Nurs |
1 |
0.11% |
| P N G Med J |
1 |
0.11% |
| Pediatr Clin North Am |
1 |
0.11% |
| Pediatr Nurs |
1 |
0.11% |
| Pediatrics |
1 |
0.11% |
| Penn Bioeth J |
1 |
0.11% |
| Perspectives Psychiatriques |
1 |
0.11% |
| Pharm Educ |
1 |
0.11% |
| Pharm J |
1 |
0.11% |
| PharmacoEconomics |
2 |
0.22% |
| Philos Ethics Humanit Med |
1 |
0.11% |
| PLoS Med |
3 |
0.32% |
| Politics Life Sci |
1 |
0.11% |
| Postgrad Med J |
2 |
0.22% |
| Prehosp Disaster Med |
1 |
0.11% |
| Presse Med |
1 |
0.11% |
| Princet J Bioeth |
1 |
0.11% |
| Proc Nutr Soc |
1 |
0.11% |
| Promotion and Education |
1 |
0.11% |
| Psychiatr Bull |
1 |
0.11% |
| Psychiatr Serv |
1 |
0.11% |
| Psychiatry |
1 |
0.11% |
| Psychiatry Clin Neurosci |
1 |
0.11% |
| Psychiatry Psychol Law |
1 |
0.11% |
| Psychiatry Psychology and Law |
1 |
0.11% |
| Public Health |
11 |
1.19% |
| Public Health Nutr |
2 |
0.22% |
| Qual Health Res |
2 |
0.22% |
| Qual Life Res |
1 |
0.11% |
| Recueil Dalloz |
1 |
0.11% |
| Reprod Health Matters |
33 |
3.56% |
| Rev Bras Psiquiatr |
1 |
0.11% |
| Rev Epidemiol Sante Publique |
1 |
0.11% |
| Rev Gaucha Enferm |
1 |
0.11% |
| Rev Lat Am Enfermagem |
3 |
0.32% |
| Rev Med Brux |
1 |
0.11% |
| Rev Med Suisse |
1 |
0.11% |
| Rev Saude Publica |
4 |
0.43% |
| Revue de droit de la santé = Tijdschrift voorgezondheidsrecht |
1 |
0.11% |
| Revue De Droit Sanitaire et Social |
3 |
0.32% |
| Revue Francophone de la Déficience Intellectuelle |
1 |
0.11% |
| S Afr J Psychiatry |
1 |
0.11% |
| S Afr J Sci |
1 |
0.11% |
| S Afr Med J |
9 |
0.97% |
| SAHARA J |
1 |
0.11% |
| Sante Ment Que |
1 |
0.11% |
| Sante Publique |
7 |
0.75% |
| Saudi Med J |
1 |
0.11% |
| Scand J Prim Health Care |
1 |
0.11% |
| Scand J Public Health |
1 |
0.11% |
| Schweizerische Ärztezeitung = Bulletin des médecins suisses |
1 |
0.11% |
| Sci Eng Ethics |
2 |
0.22% |
| Sci Sports |
1 |
0.11% |
| Sex Relatsh Ther |
1 |
0.11% |
| Soc Sci Med |
20 |
2.16% |
| South Afr J HIV Med |
1 |
0.11% |
| South Med J |
2 |
0.22% |
| Soz – Praventivmed |
1 |
0.11% |
| Stud Fam Plann |
2 |
0.22% |
| Syd Law Rev |
1 |
0.11% |
| Taiwain J Public Health |
1 |
0.11% |
| The Journal of Forensic Psychiatry |
2 |
0.22% |
| The Psychiatric Clinics of North America |
1 |
0.11% |
| Theological Studies |
1 |
0.11% |
| Theor Med Bioeth |
1 |
0.11% |
| Theor Med Bioethics |
4 |
0.43% |
| Tob Control |
4 |
0.43% |
| Trans R Soc Trop Med Hyg |
2 |
0.22% |
| Transcult Psychiatry |
2 |
0.22% |
| Transfus Clin Biol |
1 |
0.11% |
| Travail social actualités |
1 |
0.11% |
| Trends Biotechnol |
1 |
0.11% |
| Trop Doct |
1 |
0.11% |
| Urban Health |
1 |
0.11% |
| Vt Law Rev |
2 |
0.22% |
| Women Health |
1 |
0.11% |
| Women’s Health Issues |
1 |
0.11% |
| Work |
4 |
0.43% |
| World Hosp Health Serv |
1 |
0.11% |
| Z Gerontol Geriatr |
1 |
0.11% |
| Z Zagadnien Nauk Sadowych |
1 |
0.11% |
| Total |
928 |
100.00% |